Proportion of pregnant women with HBV infection eligible for antiviral prophylaxis to prevent vertical transmission: A systematic review and meta-analysis
{"title":"Proportion of pregnant women with HBV infection eligible for antiviral prophylaxis to prevent vertical transmission: A systematic review and meta-analysis","authors":"Hugues Delamare , Julian Euma Ishii-Rousseau , Adya Rao , Mélanie Cresta , Jeanne Perpétue Vincent , Olivier Ségéral , Shevanthi Nayagam , Yusuke Shimakawa","doi":"10.1016/j.jhepr.2024.101064","DOIUrl":null,"url":null,"abstract":"<div><h3>Background & Aims</h3><p>In 2020, the World Health Organization (WHO) recommended peripartum antiviral prophylaxis (PAP) for pregnant women infected with hepatitis B virus (HBV) with high viremia (≥200,000 IU/ml). Hepatitis B e antigen (HBeAg) was also recommended as an alternative when HBV DNA is unavailable. To inform policymaking and guide the implementation of prevention of mother-to-child transmission strategies, we conducted a systematic review and meta-analysis to estimate the proportion of HBV-infected pregnant women eligible for PAP at global and regional levels.</p></div><div><h3>Methods</h3><p>We searched PubMed, EMBASE, Scopus, and CENTRAL for studies involving HBV-infected pregnant women. We extracted proportions of women with high viremia (≥200,000 IU/ml), proportions of women with positive HBeAg, proportions of women cross-stratified based on HBV DNA and HBeAg, and the risk of child infection in these maternal groups. Proportions were pooled using random-effects meta-analysis.</p></div><div><h3>Results</h3><p>Of 6,999 articles, 131 studies involving 71,712 HBV-infected pregnant women were included. The number of studies per WHO region was 66 (Western Pacific), 21 (Europe), 17 (Africa), 11 (Americas), nine (Eastern Mediterranean), and seven (South-East Asia). The overall pooled proportion of high viremia was 21.27% (95% CI 17.77–25.26%), with significant regional variation: Western Pacific (31.56%), Americas (23.06%), Southeast Asia (15.62%), Africa (12.45%), Europe (9.98%), and Eastern Mediterranean (7.81%). HBeAg positivity showed similar regional variation. After cross-stratification, the proportions of high viremia and positive HBeAg, high viremia and negative HBeAg, low viremia and positive HBeAg, and low viremia and negative HBeAg were 15.24% (95% CI 11.12–20.53%), 2.70% (95% CI 1.88–3.86%), 3.69% (95% CI 2.86–4.75%), and 75.59% (95% CI 69.15–81.05%), respectively. The corresponding risks of child infection following birth dose vaccination without immune globulin and PAP were 14.86% (95% CI 8.43–24.88%), 6.94% (95% CI 2.92–15.62%), 7.14% (95% CI 1.00–37.03%), and 0.14% (95% CI 0.02–1.00%).</p></div><div><h3>Conclusions</h3><p>Approximately 20% of HBV-infected pregnant women are eligible for PAP. Given significant regional variations, each country should tailor strategies for HBsAg screening, risk stratification, and PAP in routine antenatal care.</p></div><div><h3>Impact and implications</h3><p>In 2020, the WHO recommended that pregnant women who test positive for the hepatitis B surface antigen (HBsAg) undergo HBV DNA testing or HBeAg and those with high viremia (≥200,000 IU/ml) or positive HBeAg receive PAP. To effectively implement new HBV PMTCT interventions and integrate HBV screening, risk stratification, and antiviral prophylaxis into routine antenatal care services, estimating the proportion of HBV-infected pregnant women eligible for PAP is critical. In this systematic review and meta-analysis, we found that approximately one-fifth of HBV-infected pregnant women are eligible for PAP based on HBV DNA testing, and a similar proportion is eligible based on HBeAg testing. Owing to substantial regional variations in eligibility proportions and the availability and costs of different tests, it is vital for each country to optimize strategies that integrate HBV screening, risk stratification, and PAP into routine antenatal care services.</p></div><div><h3>Systematic review registration</h3><p>This study was registered with PROSPERO (Protocol No: CRD42021266545).</p></div>","PeriodicalId":14764,"journal":{"name":"JHEP Reports","volume":"6 8","pages":"Article 101064"},"PeriodicalIF":7.5000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S258955592400065X/pdfft?md5=2027dfd80a36564806dff90afbecec17&pid=1-s2.0-S258955592400065X-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JHEP Reports","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S258955592400065X","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/26 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background & Aims
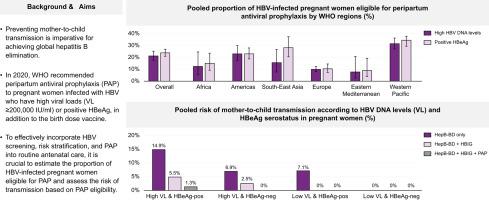
In 2020, the World Health Organization (WHO) recommended peripartum antiviral prophylaxis (PAP) for pregnant women infected with hepatitis B virus (HBV) with high viremia (≥200,000 IU/ml). Hepatitis B e antigen (HBeAg) was also recommended as an alternative when HBV DNA is unavailable. To inform policymaking and guide the implementation of prevention of mother-to-child transmission strategies, we conducted a systematic review and meta-analysis to estimate the proportion of HBV-infected pregnant women eligible for PAP at global and regional levels.
Methods
We searched PubMed, EMBASE, Scopus, and CENTRAL for studies involving HBV-infected pregnant women. We extracted proportions of women with high viremia (≥200,000 IU/ml), proportions of women with positive HBeAg, proportions of women cross-stratified based on HBV DNA and HBeAg, and the risk of child infection in these maternal groups. Proportions were pooled using random-effects meta-analysis.
Results
Of 6,999 articles, 131 studies involving 71,712 HBV-infected pregnant women were included. The number of studies per WHO region was 66 (Western Pacific), 21 (Europe), 17 (Africa), 11 (Americas), nine (Eastern Mediterranean), and seven (South-East Asia). The overall pooled proportion of high viremia was 21.27% (95% CI 17.77–25.26%), with significant regional variation: Western Pacific (31.56%), Americas (23.06%), Southeast Asia (15.62%), Africa (12.45%), Europe (9.98%), and Eastern Mediterranean (7.81%). HBeAg positivity showed similar regional variation. After cross-stratification, the proportions of high viremia and positive HBeAg, high viremia and negative HBeAg, low viremia and positive HBeAg, and low viremia and negative HBeAg were 15.24% (95% CI 11.12–20.53%), 2.70% (95% CI 1.88–3.86%), 3.69% (95% CI 2.86–4.75%), and 75.59% (95% CI 69.15–81.05%), respectively. The corresponding risks of child infection following birth dose vaccination without immune globulin and PAP were 14.86% (95% CI 8.43–24.88%), 6.94% (95% CI 2.92–15.62%), 7.14% (95% CI 1.00–37.03%), and 0.14% (95% CI 0.02–1.00%).
Conclusions
Approximately 20% of HBV-infected pregnant women are eligible for PAP. Given significant regional variations, each country should tailor strategies for HBsAg screening, risk stratification, and PAP in routine antenatal care.
Impact and implications
In 2020, the WHO recommended that pregnant women who test positive for the hepatitis B surface antigen (HBsAg) undergo HBV DNA testing or HBeAg and those with high viremia (≥200,000 IU/ml) or positive HBeAg receive PAP. To effectively implement new HBV PMTCT interventions and integrate HBV screening, risk stratification, and antiviral prophylaxis into routine antenatal care services, estimating the proportion of HBV-infected pregnant women eligible for PAP is critical. In this systematic review and meta-analysis, we found that approximately one-fifth of HBV-infected pregnant women are eligible for PAP based on HBV DNA testing, and a similar proportion is eligible based on HBeAg testing. Owing to substantial regional variations in eligibility proportions and the availability and costs of different tests, it is vital for each country to optimize strategies that integrate HBV screening, risk stratification, and PAP into routine antenatal care services.
Systematic review registration
This study was registered with PROSPERO (Protocol No: CRD42021266545).
期刊介绍:
JHEP Reports is an open access journal that is affiliated with the European Association for the Study of the Liver (EASL). It serves as a companion journal to the highly respected Journal of Hepatology.
The primary objective of JHEP Reports is to publish original papers and reviews that contribute to the advancement of knowledge in the field of liver diseases. The journal covers a wide range of topics, including basic, translational, and clinical research. It also focuses on global issues in hepatology, with particular emphasis on areas such as clinical trials, novel diagnostics, precision medicine and therapeutics, cancer research, cellular and molecular studies, artificial intelligence, microbiome research, epidemiology, and cutting-edge technologies.
In summary, JHEP Reports is dedicated to promoting scientific discoveries and innovations in liver diseases through the publication of high-quality research papers and reviews covering various aspects of hepatology.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
