{"title":"Incremental value of diastolic wall strain in predicting heart failure events in patients with atrial fibrillation","authors":"Naoki Taniguchi, Yoko Miyasaka, Yoshinobu Suwa, Eri Nakai, Shoko Harada, Hiromi Otagaki, Ichiro Shiojima","doi":"10.1007/s00380-024-02401-w","DOIUrl":null,"url":null,"abstract":"<p>Diastolic wall strain (DWS), an echocardiographic index based on linear elasticity theory, has been identified as a predictor of heart failure (HF) in patients with sinus rhythm. However, its effectiveness in atrial fibrillation (AF) patients remains uncertain. This study aims to assess DWS as a predictor of HF in AF patients with preserved ejection fraction. We analysed a prospective database of AF patients undergoing transthoracic echocardiography. AF patients with reduced left ventricular ejection fraction (< 50%), posterior wall motion abnormality, hypertrophic cardiomyopathy, valvular heart disease, pericardial disease, congenital heart disease, or history of pacemaker/implantable cardioverter-defibrillator implantation or cardiac surgery were excluded. The study followed patients until HF development, death, or last visit. Follow-up for patients who underwent catheter ablation was censored on the date of their procedure. HF was ascertained based on the Framingham criteria. DWS was calculated using a validated formula: DWS = (PWs -PWd)/PWs, where PWs is the posterior wall thickness at end-systole and PWd is the posterior wall thickness at end-diastole. Among 411 study patients (mean age 69.6 years, 66% men), 20 (5%) was underwent catheter ablation and 57 (14%) developed HF during a mean follow-up of 82 months. Cox-proportional hazards demonstrated that low DWS (≤ 0.33) significantly predicted HF events (hazard ratio [HR] 3.28, 95% confidence interval [CI]) 1.81–5.94, <i>P</i> < 0.0001), independent of age (per 10 years; HR 1.99, 95% CI 1.35–2.93, <i>P</i> < 0.001), indexed left ventricular mass (per 10 g/m<sup>2</sup>; HR 1.16, 95% CI 1.05–1.27, <i>P</i> < 0.01), and indexed left atrial volume (per 10 mL/m<sup>2</sup>; HR 1.14, 95% CI 1.04–1.24, <i>P</i> < 0.01). Additionally, global log-likelihood ratio chi-square statistics indicated that DWS incrementally predicts HF development beyond age, indexed left ventricular mass, and left atrial volume (<i>P</i> < 0.001).</p>","PeriodicalId":12940,"journal":{"name":"Heart and Vessels","volume":"51 1","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2024-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart and Vessels","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00380-024-02401-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
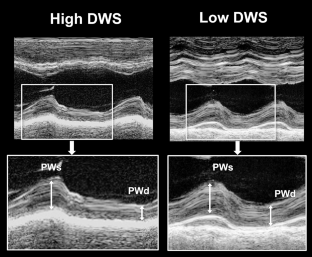
Diastolic wall strain (DWS), an echocardiographic index based on linear elasticity theory, has been identified as a predictor of heart failure (HF) in patients with sinus rhythm. However, its effectiveness in atrial fibrillation (AF) patients remains uncertain. This study aims to assess DWS as a predictor of HF in AF patients with preserved ejection fraction. We analysed a prospective database of AF patients undergoing transthoracic echocardiography. AF patients with reduced left ventricular ejection fraction (< 50%), posterior wall motion abnormality, hypertrophic cardiomyopathy, valvular heart disease, pericardial disease, congenital heart disease, or history of pacemaker/implantable cardioverter-defibrillator implantation or cardiac surgery were excluded. The study followed patients until HF development, death, or last visit. Follow-up for patients who underwent catheter ablation was censored on the date of their procedure. HF was ascertained based on the Framingham criteria. DWS was calculated using a validated formula: DWS = (PWs -PWd)/PWs, where PWs is the posterior wall thickness at end-systole and PWd is the posterior wall thickness at end-diastole. Among 411 study patients (mean age 69.6 years, 66% men), 20 (5%) was underwent catheter ablation and 57 (14%) developed HF during a mean follow-up of 82 months. Cox-proportional hazards demonstrated that low DWS (≤ 0.33) significantly predicted HF events (hazard ratio [HR] 3.28, 95% confidence interval [CI]) 1.81–5.94, P < 0.0001), independent of age (per 10 years; HR 1.99, 95% CI 1.35–2.93, P < 0.001), indexed left ventricular mass (per 10 g/m2; HR 1.16, 95% CI 1.05–1.27, P < 0.01), and indexed left atrial volume (per 10 mL/m2; HR 1.14, 95% CI 1.04–1.24, P < 0.01). Additionally, global log-likelihood ratio chi-square statistics indicated that DWS incrementally predicts HF development beyond age, indexed left ventricular mass, and left atrial volume (P < 0.001).
期刊介绍:
Heart and Vessels is an English-language journal that provides a forum of original ideas, excellent methods, and fascinating techniques on cardiovascular disease fields. All papers submitted for publication are evaluated only with regard to scientific quality and relevance to the heart and vessels. Contributions from those engaged in practical medicine, as well as from those involved in basic research, are welcomed.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
