Francesca Baciorri, Samantha Sarcognato, Francesco Di Paola, Evelina Miele, Sabrina Rossi
{"title":"A supratentorial mass in a young adult, with 25 years of follow-up","authors":"Francesca Baciorri, Samantha Sarcognato, Francesco Di Paola, Evelina Miele, Sabrina Rossi","doi":"10.1111/bpa.13260","DOIUrl":null,"url":null,"abstract":"<p>A 32-year-old male presented with a history of recent onset headaches. Imaging with magnetic resonance revealed a left parietal mass that showed heterogeneous gadolinium contrast enhancement, mild perilesional edema, and a small cystic component (Figure 1). The patient underwent surgical excision, with a complete resection of the mass. No adjuvant therapies were administered. Periodic follow-up magnetic resonance imaging did not show disease recurrence, and the patient is currently disease-free 25 years after the diagnosis (Box 1).</p><p>Histopathological examination showed a well-demarcated hypercellular neoplasm, with a multinodular growth, a rich vascular network, and perivascular paucicellular zones. The neoplastic cells displayed moderate nuclear atypia and diffuse lipomatous differentiation, which consisted of single large cytoplasmic vacuoles pushing the nuclei to the periphery of the cells, giving a signet ring appearance (Figure 2). The mitotic count reached 4 mitotic figures per 10 high-power fields, and necrosis and microvascular proliferation were absent.</p><p>By immunohistochemistry, the cells showed immunoreactivity for glial fibrillary acidic protein, S100, and focal dot-like cytoplasmic positivity for epithelial membrane antigen. Ki-67 labeling index was 10%. Electron microscopy was performed and revealed the presence of complex zipper-like intercellular junctions and microvilli, typical of ependymal differentiation (Figure 2). Twenty-five years later, the case was re-evaluated with additional immunostains and molecular analyses. The tumor proved positive for p65 and L1CAM, consistent with the diagnosis of supratentorial ependymoma, ZFTA fusion-positive (ST-EPN-ZFTA). While we failed to obtain good quality RNA for gene fusion investigation, we were able to perform DNA methylation analysis (Epic Illumina) on the original samples. In agreement with the pathological and immunohistochemical findings, the lesion classified as a ST-EPN-ZFTA (score 0.62), subtype A (score 0.58, DKFZ Classifier version v12.5). The copy number variation (CNV) profile obtained from DNA methylation analysis showed considerable background noise likely due to the age of the material; nevertheless, loss of chromosomes 9 and 22 was clearly observed (Figure 2).</p><p>Back in the days, a diagnosis of ependymoma with lipomatous differentiation, grade II, was made with the support of morphology, immunohistochemistry, and electron microscopy. After 25 years, the addition of new immunohistochemical markers and the DNA methylation profile confirmed the diagnosis and led to a more accurate definition of the lesion as a ST-EPN-ZFTA with diffuse lipomatous differentiation, grade 2.</p><p>We herein describe a case of ST-EPN-ZFTA with lipomatous differentiation arising in a young adult who did not show any recurrence over a follow-up period of 25 years. Lipomatous differentiation is described in a few central nervous system (CNS) tumors, such as medulloblastomas, central neurocytomas, and other embryonal tumors [<span>1</span>]. The occurrence of this phenomenon in ependymal neoplasms was first reported by Ruchoux et al. [<span>1</span>], when they described three cases in which tumor cells contained fat droplets, mimicking true adipocytes, while still expressing conventional immunohistochemical ependymal markers. A few additional cases with similar morphological features have been subsequently described [<span>2, 3</span>]. Notably, the large majority of them (6/9) were supratentorial [<span>1-3</span>]. Unfortunately, data on their molecular characteristics were not provided. However, based on their prevalent occurrence in the supratentorial compartment, and in light of our case, it may be speculated that lipomatous differentiation may be a rare feature in ST-EPN-ZFTA. The differential diagnosis is challenging, and includes all other CNS entities with true lipomatous differentiation. It is important to differentiate it from xanthomatous and clear cell observed in several tumors [<span>2</span>]. The main differential diagnosis is liponeurocytoma, characterized by the presence of lipid-laden cells resembling adipocytes, representing neuroepithelial tumor cells with lipid accumulation.</p><p>It is thought that the process of fat accumulation in CNS tumors may be due to divergent cell differentiation, disturbed metabolic environment or degenerative processes, instead of true metaplastic change. Gaur et al. suggested that the lipomatous differentiation in ependymoma might be ascribed to neural–mesenchymal transition of a putative pluripotent precursor cell population in the neoplasm [<span>2, 3</span>]. The prognostic role of lipomatous differentiation in ependymomas is still unknown, and most of the few cases described in the literature so far had limited follow-up periods [<span>2, 3</span>].</p><p>ST-EPN-ZFTAs, initially described as highly malignant tumors with a 10-year progression-free survival of 19%, have more recently acknowledged showing good survival rates, unless <i>CDKN2A</i> homozygous deletion is present. The CNV profile of our case was characterized by the loss of a copy of chromosome 9, but the presence of a small deletion in the other <i>CDKN2A</i> allele could not be excluded with certainty, due to the background noise depending on the old age of the material. Our patient is still disease-free 25 years after the diagnosis, representing a remarkable example of ST-EPN-ZFTA with excellent outcome.</p><p>FB and SS wrote the draft. SR, EM, and FDP reviewed and edited the draft.</p><p>The authors declare no conflicts of interest.</p><p>All data related to this case are deidentified.</p>","PeriodicalId":9290,"journal":{"name":"Brain Pathology","volume":"34 4","pages":""},"PeriodicalIF":6.2000,"publicationDate":"2024-04-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bpa.13260","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Pathology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bpa.13260","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
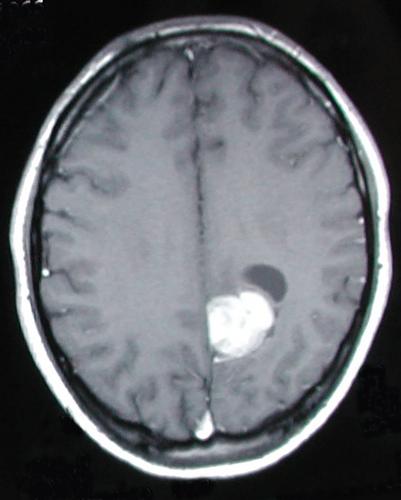
A 32-year-old male presented with a history of recent onset headaches. Imaging with magnetic resonance revealed a left parietal mass that showed heterogeneous gadolinium contrast enhancement, mild perilesional edema, and a small cystic component (Figure 1). The patient underwent surgical excision, with a complete resection of the mass. No adjuvant therapies were administered. Periodic follow-up magnetic resonance imaging did not show disease recurrence, and the patient is currently disease-free 25 years after the diagnosis (Box 1).
Histopathological examination showed a well-demarcated hypercellular neoplasm, with a multinodular growth, a rich vascular network, and perivascular paucicellular zones. The neoplastic cells displayed moderate nuclear atypia and diffuse lipomatous differentiation, which consisted of single large cytoplasmic vacuoles pushing the nuclei to the periphery of the cells, giving a signet ring appearance (Figure 2). The mitotic count reached 4 mitotic figures per 10 high-power fields, and necrosis and microvascular proliferation were absent.
By immunohistochemistry, the cells showed immunoreactivity for glial fibrillary acidic protein, S100, and focal dot-like cytoplasmic positivity for epithelial membrane antigen. Ki-67 labeling index was 10%. Electron microscopy was performed and revealed the presence of complex zipper-like intercellular junctions and microvilli, typical of ependymal differentiation (Figure 2). Twenty-five years later, the case was re-evaluated with additional immunostains and molecular analyses. The tumor proved positive for p65 and L1CAM, consistent with the diagnosis of supratentorial ependymoma, ZFTA fusion-positive (ST-EPN-ZFTA). While we failed to obtain good quality RNA for gene fusion investigation, we were able to perform DNA methylation analysis (Epic Illumina) on the original samples. In agreement with the pathological and immunohistochemical findings, the lesion classified as a ST-EPN-ZFTA (score 0.62), subtype A (score 0.58, DKFZ Classifier version v12.5). The copy number variation (CNV) profile obtained from DNA methylation analysis showed considerable background noise likely due to the age of the material; nevertheless, loss of chromosomes 9 and 22 was clearly observed (Figure 2).
Back in the days, a diagnosis of ependymoma with lipomatous differentiation, grade II, was made with the support of morphology, immunohistochemistry, and electron microscopy. After 25 years, the addition of new immunohistochemical markers and the DNA methylation profile confirmed the diagnosis and led to a more accurate definition of the lesion as a ST-EPN-ZFTA with diffuse lipomatous differentiation, grade 2.
We herein describe a case of ST-EPN-ZFTA with lipomatous differentiation arising in a young adult who did not show any recurrence over a follow-up period of 25 years. Lipomatous differentiation is described in a few central nervous system (CNS) tumors, such as medulloblastomas, central neurocytomas, and other embryonal tumors [1]. The occurrence of this phenomenon in ependymal neoplasms was first reported by Ruchoux et al. [1], when they described three cases in which tumor cells contained fat droplets, mimicking true adipocytes, while still expressing conventional immunohistochemical ependymal markers. A few additional cases with similar morphological features have been subsequently described [2, 3]. Notably, the large majority of them (6/9) were supratentorial [1-3]. Unfortunately, data on their molecular characteristics were not provided. However, based on their prevalent occurrence in the supratentorial compartment, and in light of our case, it may be speculated that lipomatous differentiation may be a rare feature in ST-EPN-ZFTA. The differential diagnosis is challenging, and includes all other CNS entities with true lipomatous differentiation. It is important to differentiate it from xanthomatous and clear cell observed in several tumors [2]. The main differential diagnosis is liponeurocytoma, characterized by the presence of lipid-laden cells resembling adipocytes, representing neuroepithelial tumor cells with lipid accumulation.
It is thought that the process of fat accumulation in CNS tumors may be due to divergent cell differentiation, disturbed metabolic environment or degenerative processes, instead of true metaplastic change. Gaur et al. suggested that the lipomatous differentiation in ependymoma might be ascribed to neural–mesenchymal transition of a putative pluripotent precursor cell population in the neoplasm [2, 3]. The prognostic role of lipomatous differentiation in ependymomas is still unknown, and most of the few cases described in the literature so far had limited follow-up periods [2, 3].
ST-EPN-ZFTAs, initially described as highly malignant tumors with a 10-year progression-free survival of 19%, have more recently acknowledged showing good survival rates, unless CDKN2A homozygous deletion is present. The CNV profile of our case was characterized by the loss of a copy of chromosome 9, but the presence of a small deletion in the other CDKN2A allele could not be excluded with certainty, due to the background noise depending on the old age of the material. Our patient is still disease-free 25 years after the diagnosis, representing a remarkable example of ST-EPN-ZFTA with excellent outcome.
FB and SS wrote the draft. SR, EM, and FDP reviewed and edited the draft.
期刊介绍:
Brain Pathology is the journal of choice for biomedical scientists investigating diseases of the nervous system. The official journal of the International Society of Neuropathology, Brain Pathology is a peer-reviewed quarterly publication that includes original research, review articles and symposia focuses on the pathogenesis of neurological disease.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
