Ivana Clark, Phoebe Wallman, Siobhan Gee, David Taylor
{"title":"Long term impact of 3-monthly paliperidone palmitate on hospitalisation in patients with schizophrenia: Six-year mirror image study","authors":"Ivana Clark, Phoebe Wallman, Siobhan Gee, David Taylor","doi":"10.1111/acps.13691","DOIUrl":null,"url":null,"abstract":"<p>Long-acting antipsychotics are accepted to be more effective than oral antipsychotics in reducing the risk of hospitalisation and relapse in schizophrenia. In our previous 5-year mirror-image study, we reported a significant reduction in hospital admissions and fewer days spent in hospital for people prescribed 3-monthly paliperidone (PP3M) after stabilisation on 1-monthly (PP1M).<span><sup>1</sup></span> We now report the outcomes of the sixth year of this study.</p><p>Our primary objective was to use a mirror image model to evaluate hospital admissions and bed days before and after the initiation of PP1M followed by PP3M in those who continued treatment for 3 years. Full details of methods used have been previously described.<span><sup>1</sup></span> The same patient cohort as previously defined was followed up for additional 12 months.</p><p>As before, 76 patients met inclusion criteria. Of this total baseline cohort, 52 patients (68%) continued on PPLAIs for 36 months, 19 patients (25%) discontinued within 36 months of initiation and 5 patients (7%) were lost to follow-up. The mean age on PPLAI initiation was 42 years; 54 were male. The majority of our baseline cohort was initiated on PP1M as inpatients (<i>n</i> = 49, 69%). Ethnicity breakdown was as follows: Asian (<i>n</i> = 4), Black (<i>n</i> = 44), Mixed background (<i>n</i> = 4), Other (<i>n</i> = 2), White (<i>n</i> = 17). On average, patients received PP1M for 10 months before starting PP3M. The most commonly prescribed maintenance dose was 100 mg a month (<i>n</i> = 31 [44%]) followed by 150 mg (<i>n</i> = 25, 35%), 75 mg (<i>n</i> = 12, 17%) and 50 mg (<i>n</i> = 3, 4%). From the original 76 starters, 19 patients discontinued over 36 months, for the following reasons: patient refusal (<i>n</i> = 10), perceived inefficacy (<i>n</i> = 5), unrelated health condition (‘kidney problems’ [<i>n</i> = 1] and cancer [<i>n</i> = 1]) and adverse effects (weight gain [<i>n</i> = 1] and raised liver function tests [<i>n</i> = 1]).</p><p>In those continuing on PPLAI for 3 years (<i>n</i> = 52), the mean number of admissions per year was 0.53 (SD 0.49) before PPLAI initiation and 0.01 (SD 0.06) (<i>p</i> < 0.001) afterwards. The mean number of bed days a year was 31.3 days (SD 48.8) before PPLAI and 12.4 days (SD 23.6) (<i>p</i> < 0.001) after. The majority of the bed days recorded in the period after PPLAI was started were from the index admission. Only two patients registered bed days after initiation (discounting the initial admission bed days). Both patients started PPLAI as inpatients. No patient starting PPLAI as an out-patient had bed days in the 3 years after initiation.</p><p>The use of PP3M after stabilisation on PP1M was associated with a considerable reduction in bed days and hospital admissions. During the observational period, only 8 of 71 patients started on PP1M/3 M (9.9%) were admitted to hospital. The majority of our patient cohort (80%) had been admitted to hospital at least once in the 3 years before starting PP1M. The mean number of admissions per year decreased by 98% in those continuing for 3 years. There were no admissions to the hospital in people continuing on PP3M for the last 18 months of the observational period. This is remarkable outcome when one considers that these patients were so frequently hospitalised before switching to PP3M.</p><p>The average number of bed days per year after the initiation of PPLAIs was reduced by more than half but a significant proportion of bed days recorded after starting PP1M was attributed to the initial or index admission. Patients who remained on treatment throughout the observational period showed a steady decrease in bed days, reaching zero days by the third year of treatment (mean bed days fell from 39.8 in year 1 to 0.63 in year 2 and to 0.0 in year 3) (Figure 1). The absence of bed days in the third year for continuers indicates that assured delivery of effective antipsychotic treatment can effectively reduce the risk of psychotic relapse to zero.</p><p>In the United Kingdom, the average annual cost of a standard bed is £125,925.<span><sup>2</sup></span> In this study, the mean number of days spent in hospital reduced by an average 18.9 days/person/year for those continuing. This equates to cost savings £6521 per year. The yearly cost for the maximum dose of PP3M (525 mg) is £4711.<span><sup>3</sup></span> However, the majority of our cohort were prescribed 350 mg PP3M. Using the cost for this dose net yearly savings were £2752. It is also important to highlight the additional benefits of less frequent administration such as a reduction in staff time devoted to injection procedures, increased patient activity and involvement in the community, improved social relationships and decreased feeling of stigma owing to schizophrenia diagnosis.<span><sup>4</sup></span></p><p>DT reports research funding from Janssen and speaker's honoraria from Janssen, Otsuka, Viatris and Recordati. IC, PW and SG declare none.</p>","PeriodicalId":108,"journal":{"name":"Acta Psychiatrica Scandinavica","volume":"150 1","pages":"48-50"},"PeriodicalIF":5.0000,"publicationDate":"2024-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/acps.13691","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Psychiatrica Scandinavica","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/acps.13691","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Long-acting antipsychotics are accepted to be more effective than oral antipsychotics in reducing the risk of hospitalisation and relapse in schizophrenia. In our previous 5-year mirror-image study, we reported a significant reduction in hospital admissions and fewer days spent in hospital for people prescribed 3-monthly paliperidone (PP3M) after stabilisation on 1-monthly (PP1M).1 We now report the outcomes of the sixth year of this study.
Our primary objective was to use a mirror image model to evaluate hospital admissions and bed days before and after the initiation of PP1M followed by PP3M in those who continued treatment for 3 years. Full details of methods used have been previously described.1 The same patient cohort as previously defined was followed up for additional 12 months.
As before, 76 patients met inclusion criteria. Of this total baseline cohort, 52 patients (68%) continued on PPLAIs for 36 months, 19 patients (25%) discontinued within 36 months of initiation and 5 patients (7%) were lost to follow-up. The mean age on PPLAI initiation was 42 years; 54 were male. The majority of our baseline cohort was initiated on PP1M as inpatients (n = 49, 69%). Ethnicity breakdown was as follows: Asian (n = 4), Black (n = 44), Mixed background (n = 4), Other (n = 2), White (n = 17). On average, patients received PP1M for 10 months before starting PP3M. The most commonly prescribed maintenance dose was 100 mg a month (n = 31 [44%]) followed by 150 mg (n = 25, 35%), 75 mg (n = 12, 17%) and 50 mg (n = 3, 4%). From the original 76 starters, 19 patients discontinued over 36 months, for the following reasons: patient refusal (n = 10), perceived inefficacy (n = 5), unrelated health condition (‘kidney problems’ [n = 1] and cancer [n = 1]) and adverse effects (weight gain [n = 1] and raised liver function tests [n = 1]).
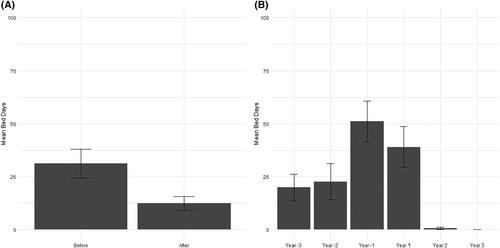
In those continuing on PPLAI for 3 years (n = 52), the mean number of admissions per year was 0.53 (SD 0.49) before PPLAI initiation and 0.01 (SD 0.06) (p < 0.001) afterwards. The mean number of bed days a year was 31.3 days (SD 48.8) before PPLAI and 12.4 days (SD 23.6) (p < 0.001) after. The majority of the bed days recorded in the period after PPLAI was started were from the index admission. Only two patients registered bed days after initiation (discounting the initial admission bed days). Both patients started PPLAI as inpatients. No patient starting PPLAI as an out-patient had bed days in the 3 years after initiation.
The use of PP3M after stabilisation on PP1M was associated with a considerable reduction in bed days and hospital admissions. During the observational period, only 8 of 71 patients started on PP1M/3 M (9.9%) were admitted to hospital. The majority of our patient cohort (80%) had been admitted to hospital at least once in the 3 years before starting PP1M. The mean number of admissions per year decreased by 98% in those continuing for 3 years. There were no admissions to the hospital in people continuing on PP3M for the last 18 months of the observational period. This is remarkable outcome when one considers that these patients were so frequently hospitalised before switching to PP3M.
The average number of bed days per year after the initiation of PPLAIs was reduced by more than half but a significant proportion of bed days recorded after starting PP1M was attributed to the initial or index admission. Patients who remained on treatment throughout the observational period showed a steady decrease in bed days, reaching zero days by the third year of treatment (mean bed days fell from 39.8 in year 1 to 0.63 in year 2 and to 0.0 in year 3) (Figure 1). The absence of bed days in the third year for continuers indicates that assured delivery of effective antipsychotic treatment can effectively reduce the risk of psychotic relapse to zero.
In the United Kingdom, the average annual cost of a standard bed is £125,925.2 In this study, the mean number of days spent in hospital reduced by an average 18.9 days/person/year for those continuing. This equates to cost savings £6521 per year. The yearly cost for the maximum dose of PP3M (525 mg) is £4711.3 However, the majority of our cohort were prescribed 350 mg PP3M. Using the cost for this dose net yearly savings were £2752. It is also important to highlight the additional benefits of less frequent administration such as a reduction in staff time devoted to injection procedures, increased patient activity and involvement in the community, improved social relationships and decreased feeling of stigma owing to schizophrenia diagnosis.4
DT reports research funding from Janssen and speaker's honoraria from Janssen, Otsuka, Viatris and Recordati. IC, PW and SG declare none.
期刊介绍:
Acta Psychiatrica Scandinavica acts as an international forum for the dissemination of information advancing the science and practice of psychiatry. In particular we focus on communicating frontline research to clinical psychiatrists and psychiatric researchers.
Acta Psychiatrica Scandinavica has traditionally been and remains a journal focusing predominantly on clinical psychiatry, but translational psychiatry is a topic of growing importance to our readers. Therefore, the journal welcomes submission of manuscripts based on both clinical- and more translational (e.g. preclinical and epidemiological) research. When preparing manuscripts based on translational studies for submission to Acta Psychiatrica Scandinavica, the authors should place emphasis on the clinical significance of the research question and the findings. Manuscripts based solely on preclinical research (e.g. animal models) are normally not considered for publication in the Journal.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
