Isa F. Ashoor, Rachel M. Engen, Dechu Puliyanda, Nicole Hayde, Caitlin G. Peterson, Rima S. Zahr, Sonia Solomon, Mahmoud Kallash, Rouba Garro, Amrish Jain, Lyndsay A. Harshman, Scott T. McEwen, Asifhusen Mansuri, Mathew J. Gregoski, Katherine E. Twombley
{"title":"Antibody‐mediated rejection in pediatric kidney transplant recipients: A report from the Pediatric Nephrology Research Consortium","authors":"Isa F. Ashoor, Rachel M. Engen, Dechu Puliyanda, Nicole Hayde, Caitlin G. Peterson, Rima S. Zahr, Sonia Solomon, Mahmoud Kallash, Rouba Garro, Amrish Jain, Lyndsay A. Harshman, Scott T. McEwen, Asifhusen Mansuri, Mathew J. Gregoski, Katherine E. Twombley","doi":"10.1111/petr.14734","DOIUrl":null,"url":null,"abstract":"BackgroundAntibody‐mediated rejection (AMR) is a major cause of kidney allograft loss. There is a paucity of large‐scale pediatric‐specific data regarding AMR treatment outcomes.MethodsData were obtained from 14 centers within the Pediatric Nephrology Research Consortium. Kidney transplant recipients aged 1–18 years at transplant with biopsy‐proven AMR between 2009 and 2019 and at least 12 months of follow‐up were included. The primary outcome was graft failure or an eGFR <20 mL/min/1.73 m<jats:sup>2</jats:sup> at 12 months following AMR treatment. AMR treatment choice, histopathology, and DSA class were also examined.ResultsWe reviewed 123 AMR episodes. Median age at diagnosis was 15 years at a median 22 months post‐transplant. The primary outcome developed in 27.6%. eGFR <30 m/min/1.73 m<jats:sup>2</jats:sup> at AMR diagnosis was associated with a 5.6‐fold higher risk of reaching the composite outcome. There were no significant differences in outcome by treatment modality. Histopathology scores and DSA class at time of AMR diagnosis were not significantly associated with the primary outcome.ConclusionsIn this large cohort of pediatric kidney transplant recipients with AMR, nearly one‐third of patients experienced graft failure or significant graft dysfunction within 12 months of diagnosis. Poor graft function at time of diagnosis was associated with higher odds of graft failure.","PeriodicalId":20038,"journal":{"name":"Pediatric Transplantation","volume":"85 1","pages":""},"PeriodicalIF":1.4000,"publicationDate":"2024-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/petr.14734","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
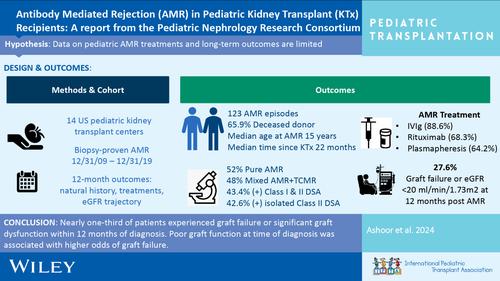
BackgroundAntibody‐mediated rejection (AMR) is a major cause of kidney allograft loss. There is a paucity of large‐scale pediatric‐specific data regarding AMR treatment outcomes.MethodsData were obtained from 14 centers within the Pediatric Nephrology Research Consortium. Kidney transplant recipients aged 1–18 years at transplant with biopsy‐proven AMR between 2009 and 2019 and at least 12 months of follow‐up were included. The primary outcome was graft failure or an eGFR <20 mL/min/1.73 m2 at 12 months following AMR treatment. AMR treatment choice, histopathology, and DSA class were also examined.ResultsWe reviewed 123 AMR episodes. Median age at diagnosis was 15 years at a median 22 months post‐transplant. The primary outcome developed in 27.6%. eGFR <30 m/min/1.73 m2 at AMR diagnosis was associated with a 5.6‐fold higher risk of reaching the composite outcome. There were no significant differences in outcome by treatment modality. Histopathology scores and DSA class at time of AMR diagnosis were not significantly associated with the primary outcome.ConclusionsIn this large cohort of pediatric kidney transplant recipients with AMR, nearly one‐third of patients experienced graft failure or significant graft dysfunction within 12 months of diagnosis. Poor graft function at time of diagnosis was associated with higher odds of graft failure.
期刊介绍:
The aim of Pediatric Transplantation is to publish original articles of the highest quality on clinical experience and basic research in transplantation of tissues and solid organs in infants, children and adolescents. The journal seeks to disseminate the latest information widely to all individuals involved in kidney, liver, heart, lung, intestine and stem cell (bone-marrow) transplantation. In addition, the journal publishes focused reviews on topics relevant to pediatric transplantation as well as timely editorial comment on controversial issues.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
