{"title":"Laparoscopic versus open parenchymal sparing liver resections for high tumour burden colorectal liver metastases: a propensity score matched analysis","authors":"Nadia Russolillo, Cristina Ciulli, Caterina Costanza Zingaretti, Andrea Pierluigi Fontana, Serena Langella, Alessandro Ferrero","doi":"10.1007/s00464-024-10797-9","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background</h3><p>Laparoscopic liver resection (LLR) has proved effective in the treatment of oligometastatic disease (1 or 2 colorectal liver metastases CRLM) with similar long-term outcomes and improved short-term results compared to open liver resection (OLR). Feasibility of parenchymal sparing LLR for high tumour burden diseases is largely unknown. Aim of the study was to compare short and long-term results of LLR and OLR in patients with ≥ 3 CRLM.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>Patients who underwent first LR of at least two different segments for ≥ 3 CRLM between 01/2012 and 12/2021 were analysed. Propensity score nearest-neighbour 1:1 matching was based on relevant prognostic factors.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>277 out of 673 patients fulfilled inclusion criteria (47 LLR and 230 OLR). After match two balanced groups of 47 patients with a similar mean number of CRLM (5 in LLR vs 6.5 in OLR, <i>p</i> = 0.170) were analysed. The rate of major hepatectomy was similar between the two group (10.6% OLR vs. 12.8% LLR). Mortality (2.1% OLR vs 0 LLR) and overall morbidity rates (34% OLR vs 23.4% LLR) were comparable. Length of stay (LOS) was shorter in the LLR group (5 vs 9 days, <i>p</i> = 0.001). No differences were observed in median overall (41.1 months OLR vs median not reached LLR) and disease-free survival (18.3 OLR vs 27.9 months LLR).</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>Laparoscopic approach should be considered in selected patients scheduled to parenchymal sparing LR for high tumour burden disease as associated to shorter LOS and similar postoperative and long-term outcomes compared to the open approach.</p>","PeriodicalId":501625,"journal":{"name":"Surgical Endoscopy","volume":"49 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-04-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00464-024-10797-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Laparoscopic liver resection (LLR) has proved effective in the treatment of oligometastatic disease (1 or 2 colorectal liver metastases CRLM) with similar long-term outcomes and improved short-term results compared to open liver resection (OLR). Feasibility of parenchymal sparing LLR for high tumour burden diseases is largely unknown. Aim of the study was to compare short and long-term results of LLR and OLR in patients with ≥ 3 CRLM.
Methods
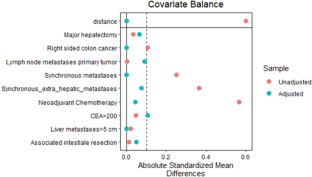
Patients who underwent first LR of at least two different segments for ≥ 3 CRLM between 01/2012 and 12/2021 were analysed. Propensity score nearest-neighbour 1:1 matching was based on relevant prognostic factors.
Results
277 out of 673 patients fulfilled inclusion criteria (47 LLR and 230 OLR). After match two balanced groups of 47 patients with a similar mean number of CRLM (5 in LLR vs 6.5 in OLR, p = 0.170) were analysed. The rate of major hepatectomy was similar between the two group (10.6% OLR vs. 12.8% LLR). Mortality (2.1% OLR vs 0 LLR) and overall morbidity rates (34% OLR vs 23.4% LLR) were comparable. Length of stay (LOS) was shorter in the LLR group (5 vs 9 days, p = 0.001). No differences were observed in median overall (41.1 months OLR vs median not reached LLR) and disease-free survival (18.3 OLR vs 27.9 months LLR).
Conclusion
Laparoscopic approach should be considered in selected patients scheduled to parenchymal sparing LR for high tumour burden disease as associated to shorter LOS and similar postoperative and long-term outcomes compared to the open approach.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
