{"title":"Ma2 antibody-associated limbic encephalitis: The early etiology treatment may modify the disease clinical trajectory","authors":"Pietro Mattioli, Stefano Grisanti, Federico Massa, Silvia Morbelli, Silvia Boni, Alessandro Beronio, Giacomo Rebella, Luca Roccatagliata, Lino Nobili, Diego Franciotta, Elisa Micalizzi, Flavio Nobili, Dario Arnaldi, Flavio Villani, Luana Benedetti","doi":"10.1002/epd2.20225","DOIUrl":null,"url":null,"abstract":"<p>Paraneoplastic encephalitis includes neurological conditions with autoantibodies against neuronal proteins, likely triggered by the underlying tumor antigens.<span><sup>1</sup></span> We report two patients with paraneoplastic limbic encephalitis<span><sup>1</sup></span> with “high-risk-for-cancer” antibodies against Ma2 antigen and non-typical tumors. These cases allow consideration of autoimmune epilepsy's pathogenesis, the importance of early diagnosis, and therapy.</p><p>A 21-year-old male admitted to the Infectious Disease Unit due to confusion, visual hallucinations, and upper limbs myoclonus, following a 4-month history of antipyretic-resistant fever, sore throat, and hyperphagia. Cerebrospinal fluid (CSF) analysis was normal, blood examinations showed pancytopenia. Brain MRI, [<sup>18</sup>F]FDG-PET, and EEG (Figure 1A–D) suggested central nervous system inflammation involving basal ganglia and mesial temporal lobes. Screening for infections was negative. Anti-Ma2 antibodies were found in serum and CSF (indirect immunofluorescence on primate cerebellum, and dot-blot; Euroimmun, Germany). IV methylprednisolone (1 g/day for 5 days) and immunoglobulins (IVIg) (.4 g/kg/day for 5 days) yielded no clinical improvement. Total body CT, [<sup>18</sup>F]FDG-PET, pelvis, and testicular ultrasound excluded neoplasms, but bone marrow analysis, 6 months after symptoms' onset, showed a clonal population of CD19/CD20dim/CD21 B lymphocytes, indicating a mature B-cell indolent lymphoproliferative disorder not requiring treatment. Hospital-acquired sepsis hindered further immunosuppressive therapies and led to death (7 months after symptoms' onset).</p><p>The second patient, a 30-year-old male, presented with asthenia, insomnia, mild fever, and daily, short-lasting episodes of shivering, horripilation, heart palpitations, and unpleasant taste. Subtle sleep-related involuntary movements were reported. No EEG was performed at the time. 1 month after symptom onset, a right testicular mass was noticed and orchiectomy performed. Pathology disclosed a post-puberal teratoma. 2 months later, a scheduled total body CT showed enlargement of retroperitoneal lymph-nodes, which were completely removed. Pathology disclosed a post-puberal teratoma with embryonal cancer focus. The patients started clinical and radiological follow-up, with no further localizations detected. 5 months later, he presented a focal-to-bilateral seizure, promptingantiseizure medications. Brain MRI and [<sup>18</sup>F]FDG-PET indicated limbic encephalitiswith EEG showing interictal epileptiform discharges in left temporal lobe (Figure 1E–H). Anti-Ma2 antibodies were detected in serum and CSF (indirect immunofluorescence on primate cerebellum, and dot-blot; Euroimmun, Germany), but not anti-NMDAR (antigen-specific cell-based assay (Euroimmun, Germany)). IVIg (.4 g/kg/day for 5 days), methylprednisolone (500 mg/day for 3 days) followed by oral prednisone (50 mg/day) led to seizure frequency reduction. IVIg cycles were repeated six times. 9 months after the first IVIg cycle, brain MRI, and [<sup>18</sup>F]FDG-PET showed reduced T2-hyperintensities of temporal lobes, but mild right temporal-mesial hypermetabolism (Figure S1). Escalation to Rituximab was required for persistent focal aware seizures with vegetative symptoms (horripilation) and mild behavioral abnormalities. At 1-year follow-up, the neurobehavioral status improved along with the persistence of sporadic clusters of focal aware seizures, responsive to oral prednisone boosts (1 mg/kg for 5 days, with subsequent weekly 10% dose tapering). Tumor recurrence in contralateral testis and in other locations were searched, but not found.</p><p>The association of Ma2 antibodies with other than testicular cancer is rare.<span><sup>2-8</sup></span> Indeed, in patient 1 the lymphoproliferative disease showed insidious presentation resulting in a 6-month diagnostic delay and was complicated by hospital-acquired sepsis, hindering second-line immunosuppressive therapies. In patient 2, the tumor was treated 1 month after symptoms onset. In agreement with literature data,<span><sup>1, 4</sup></span> early immunological treatment, along with earlier eradication of the tumor likely promoted a better prognosis. On the other hand, the persistence of focal aware seizures is consistent with a recent study on autoimmune epilepsy demonstrating frequent drug-refractory epilepsy in Ma2 patients.<span><sup>9</sup></span> Mild clinical (neurobehavioral symptoms) and neuroimaging ([<sup>18</sup>F]FDG-PET hypermetabolism reflecting mesial temporal lobes inflammation) signs of inflammation are important factors which are consistent with the hypothesis that the pathogenesis of autoimmune epilepsy in Ma2 patients may be related to persisting inflammatory process rather than the effect of chronic post-encephalitic lesion,<span><sup>9</sup></span> as it has been also suggested by a recently published case report.<span><sup>10</sup></span> Our observation advocated in our patient the use of immunotherapy to treat persisting seizures despite the long time passed from seizures' onset. Further studies, with the specific aim of identifying biomarkers of inflammation and the consequences of long-term immune treatments in such conditions are needed to confirm such speculations.</p><p>In conclusion, in line with the literature,<span><sup>1</sup></span> early etiological treatment and continuation of immunotherapy should be considered in paraneoplastic encephalitis.</p><p>Arnaldi D. received fees from Fidia for lectures and board participation; Morbelli S. has received speaker Honoraria from G.E. Healthcare; Nobili F. has received fees for participating in boards from Roche, and speaker Honoraria from Bial e G.E. Healthcare. Villani F. has received speaker's honoraria and fees for participating in boards from UCB Pharma, Angelini Pharma, EISAI, Lusofarmaco, Bial, Jazz Pharma. Micalizzi E. has received fees for participating in a board from Angelini Pharma. The other authors have nothing to disclose.</p>","PeriodicalId":50508,"journal":{"name":"Epileptic Disorders","volume":"26 3","pages":"407-411"},"PeriodicalIF":2.7000,"publicationDate":"2024-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/epd2.20225","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epileptic Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/epd2.20225","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Paraneoplastic encephalitis includes neurological conditions with autoantibodies against neuronal proteins, likely triggered by the underlying tumor antigens.1 We report two patients with paraneoplastic limbic encephalitis1 with “high-risk-for-cancer” antibodies against Ma2 antigen and non-typical tumors. These cases allow consideration of autoimmune epilepsy's pathogenesis, the importance of early diagnosis, and therapy.
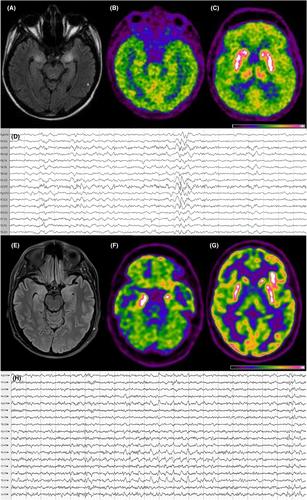
A 21-year-old male admitted to the Infectious Disease Unit due to confusion, visual hallucinations, and upper limbs myoclonus, following a 4-month history of antipyretic-resistant fever, sore throat, and hyperphagia. Cerebrospinal fluid (CSF) analysis was normal, blood examinations showed pancytopenia. Brain MRI, [18F]FDG-PET, and EEG (Figure 1A–D) suggested central nervous system inflammation involving basal ganglia and mesial temporal lobes. Screening for infections was negative. Anti-Ma2 antibodies were found in serum and CSF (indirect immunofluorescence on primate cerebellum, and dot-blot; Euroimmun, Germany). IV methylprednisolone (1 g/day for 5 days) and immunoglobulins (IVIg) (.4 g/kg/day for 5 days) yielded no clinical improvement. Total body CT, [18F]FDG-PET, pelvis, and testicular ultrasound excluded neoplasms, but bone marrow analysis, 6 months after symptoms' onset, showed a clonal population of CD19/CD20dim/CD21 B lymphocytes, indicating a mature B-cell indolent lymphoproliferative disorder not requiring treatment. Hospital-acquired sepsis hindered further immunosuppressive therapies and led to death (7 months after symptoms' onset).
The second patient, a 30-year-old male, presented with asthenia, insomnia, mild fever, and daily, short-lasting episodes of shivering, horripilation, heart palpitations, and unpleasant taste. Subtle sleep-related involuntary movements were reported. No EEG was performed at the time. 1 month after symptom onset, a right testicular mass was noticed and orchiectomy performed. Pathology disclosed a post-puberal teratoma. 2 months later, a scheduled total body CT showed enlargement of retroperitoneal lymph-nodes, which were completely removed. Pathology disclosed a post-puberal teratoma with embryonal cancer focus. The patients started clinical and radiological follow-up, with no further localizations detected. 5 months later, he presented a focal-to-bilateral seizure, promptingantiseizure medications. Brain MRI and [18F]FDG-PET indicated limbic encephalitiswith EEG showing interictal epileptiform discharges in left temporal lobe (Figure 1E–H). Anti-Ma2 antibodies were detected in serum and CSF (indirect immunofluorescence on primate cerebellum, and dot-blot; Euroimmun, Germany), but not anti-NMDAR (antigen-specific cell-based assay (Euroimmun, Germany)). IVIg (.4 g/kg/day for 5 days), methylprednisolone (500 mg/day for 3 days) followed by oral prednisone (50 mg/day) led to seizure frequency reduction. IVIg cycles were repeated six times. 9 months after the first IVIg cycle, brain MRI, and [18F]FDG-PET showed reduced T2-hyperintensities of temporal lobes, but mild right temporal-mesial hypermetabolism (Figure S1). Escalation to Rituximab was required for persistent focal aware seizures with vegetative symptoms (horripilation) and mild behavioral abnormalities. At 1-year follow-up, the neurobehavioral status improved along with the persistence of sporadic clusters of focal aware seizures, responsive to oral prednisone boosts (1 mg/kg for 5 days, with subsequent weekly 10% dose tapering). Tumor recurrence in contralateral testis and in other locations were searched, but not found.
The association of Ma2 antibodies with other than testicular cancer is rare.2-8 Indeed, in patient 1 the lymphoproliferative disease showed insidious presentation resulting in a 6-month diagnostic delay and was complicated by hospital-acquired sepsis, hindering second-line immunosuppressive therapies. In patient 2, the tumor was treated 1 month after symptoms onset. In agreement with literature data,1, 4 early immunological treatment, along with earlier eradication of the tumor likely promoted a better prognosis. On the other hand, the persistence of focal aware seizures is consistent with a recent study on autoimmune epilepsy demonstrating frequent drug-refractory epilepsy in Ma2 patients.9 Mild clinical (neurobehavioral symptoms) and neuroimaging ([18F]FDG-PET hypermetabolism reflecting mesial temporal lobes inflammation) signs of inflammation are important factors which are consistent with the hypothesis that the pathogenesis of autoimmune epilepsy in Ma2 patients may be related to persisting inflammatory process rather than the effect of chronic post-encephalitic lesion,9 as it has been also suggested by a recently published case report.10 Our observation advocated in our patient the use of immunotherapy to treat persisting seizures despite the long time passed from seizures' onset. Further studies, with the specific aim of identifying biomarkers of inflammation and the consequences of long-term immune treatments in such conditions are needed to confirm such speculations.
In conclusion, in line with the literature,1 early etiological treatment and continuation of immunotherapy should be considered in paraneoplastic encephalitis.
Arnaldi D. received fees from Fidia for lectures and board participation; Morbelli S. has received speaker Honoraria from G.E. Healthcare; Nobili F. has received fees for participating in boards from Roche, and speaker Honoraria from Bial e G.E. Healthcare. Villani F. has received speaker's honoraria and fees for participating in boards from UCB Pharma, Angelini Pharma, EISAI, Lusofarmaco, Bial, Jazz Pharma. Micalizzi E. has received fees for participating in a board from Angelini Pharma. The other authors have nothing to disclose.
期刊介绍:
Epileptic Disorders is the leading forum where all experts and medical studentswho wish to improve their understanding of epilepsy and related disorders can share practical experiences surrounding diagnosis and care, natural history, and management of seizures.
Epileptic Disorders is the official E-journal of the International League Against Epilepsy for educational communication. As the journal celebrates its 20th anniversary, it will now be available only as an online version. Its mission is to create educational links between epileptologists and other health professionals in clinical practice and scientists or physicians in research-based institutions. This change is accompanied by an increase in the number of issues per year, from 4 to 6, to ensure regular diffusion of recently published material (high quality Review and Seminar in Epileptology papers; Original Research articles or Case reports of educational value; MultiMedia Teaching Material), to serve the global medical community that cares for those affected by epilepsy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
