Ieva Lingytė, Paula Kaminskienė, Arūnas Petkevičius, Asta Baranauskaitė
{"title":"Upadacitinib for management of alopecia areata and rheumatoid arthritis: Letter to the editor","authors":"Ieva Lingytė, Paula Kaminskienė, Arūnas Petkevičius, Asta Baranauskaitė","doi":"10.1002/jvc2.433","DOIUrl":null,"url":null,"abstract":"<p>We present the case of a 54-year-old woman with a 14-year history of seropositive rheumatoid arthritis (RA) and 12 years of patchy alopecia areata (AA). RA presented with typical symmetric arthritis of small joints of the hands, morning stiffness lasting for more than 1 h, high rheumatoid factor (49.5 kU/L), and anti-cyclic citrullinated peptide antibodies (153.14 kU/L). The treatment of RA involved oral methotrexate at a dose of 17.5 mg per week, along with nonsteroidal anti-inflammatory drugs, prescribed in 2009. Hair loss began 2 years later, and the patient consulted a dermatologist who diagnosed AA. Since methotrexate was suitable for both diseases, no additional systemic AA treatment was prescribed at that time, and topical treatment for the scalp (0.05% clobetasol propionate and 5% minoxidil) was added. However, the topical treatment showed no effect and was discontinued after a few years. Methotrexate was changed to leflunomide at a daily dose of 20 mg due to its ineffectiveness for arthritis at the end of 2011. As RA remained active with a high Disease Activity Score-28 (DAS-28) index, reaching up to 5.43, leflunomide was stopped, and an inhibitor of tumour necrosis factor-alpha etanercept at 50 mg per week, was prescribed in 2013 and continued for 10 years. During this treatment, low disease activity of RA was maintained with short-term exacerbations, and no significant side effects were observed. The DAS-28 index ranged from 1.32 to 3.47. However, AA persisted throughout this period without significant improvement or deterioration. An exacerbation of RA and AA was noticed at the beginning of 2023, leading to the decision to stop etanercept and to start therapy with the selective Janus kinase (JAK) 1 inhibitor upadacitinib at a dose of 15 mg daily. Upadacitinib was prescribed as it was the only JAK inhibitor reimbursed in Lithuania at that time. During the visit, trichoscopy of the scalp was performed and showed broken hairs, black and yellow dots, vellus hairs, with a Severity of Alopecia Tool (SALT) score of 51 (Figure 1a). A significant improvement in RA was observed within 3 months, with the DAS-28 decreasing from 2.21 to 1.18. The hair regrew completely after 6 months with the SALT score of 0 and with no evidence of disease activity on trichoscopy (Figure 1b,c). No side effects were observed with upadacitinib, and laboratory tests performed every 3 months returned normal results.</p><p>AA is associated with autoimmune diseases such as RA due to the similar involvement of the JAK and signal transducer and activator of transcription signalling pathway (JAK/STAT).<span><sup>1, 2</sup></span> Cytokines such interferon-γ, interleukin-2 (IL-2), interleukin-7 (IL-7) and interleukin-15 (IL-15) are believed to play an important role in the pathogenesis of AA. These cytokines activate certain JAK molecules, leading to the phosphorylation of the corresponding domains of the STAT pathway. This phosphorylation ultimately leads to the transcription of the target gene.<span><sup>3</sup></span> JAK inhibitors hold promise as a new treatment for AA. In June 2022, the Food and Drug Administration (FDA) authorised baricitinib for the treatment of severe AA and in June 2023, the FDA approved another JAK inhibitor, called ritlecitinib.<span><sup>4</sup></span> However, upadacitinib and ruxolitinib have not yet been approved for the treatment of AA. Upadacitinib is a selective JAK-1 inhibitor, which blocks signalling of many inflammatory cytokines, including IL-2, IL-6, IL-7 and IL-15, suppressing the inflammation common to both diseases.<span><sup>5, 6</sup></span> Several successful cases of upadacitinib 15 or 20 mg daily in patients with AA and concomitant atopic dermatitis or Crohn's disease have been published in the literature.<span><sup>7, 8</sup></span> In this letter, we provide evidence that upadacitinib at 15 mg daily could be an effective treatment for AA in patients with RA.</p><p>Ieva Lingytė: Conception of the work; Data analysis and interpretation, Drafting the article. Paula Kaminskienė: Data analysis and interpretation, Drafting the article. Arūnas Petkevičius: Critical revision of the article, Final approval of the version to be published. Asta Baranauskaitė: Conception of the work; Data collection; Critical revision of the article; Final approval of the version to be published.</p><p>The authors declare no conflict of interest.</p><p>All patients in this manuscript have given written informed consent for participation in the study and the use of their deidentified, anonymized, aggregated data and their case details (including photographs) for publication. Ethical Approval: not applicable.</p>","PeriodicalId":94325,"journal":{"name":"JEADV clinical practice","volume":"3 4","pages":"1298-1300"},"PeriodicalIF":0.5000,"publicationDate":"2024-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jvc2.433","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JEADV clinical practice","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jvc2.433","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
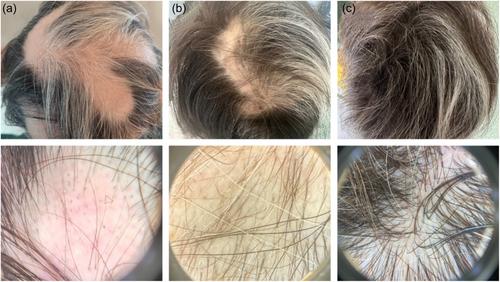
We present the case of a 54-year-old woman with a 14-year history of seropositive rheumatoid arthritis (RA) and 12 years of patchy alopecia areata (AA). RA presented with typical symmetric arthritis of small joints of the hands, morning stiffness lasting for more than 1 h, high rheumatoid factor (49.5 kU/L), and anti-cyclic citrullinated peptide antibodies (153.14 kU/L). The treatment of RA involved oral methotrexate at a dose of 17.5 mg per week, along with nonsteroidal anti-inflammatory drugs, prescribed in 2009. Hair loss began 2 years later, and the patient consulted a dermatologist who diagnosed AA. Since methotrexate was suitable for both diseases, no additional systemic AA treatment was prescribed at that time, and topical treatment for the scalp (0.05% clobetasol propionate and 5% minoxidil) was added. However, the topical treatment showed no effect and was discontinued after a few years. Methotrexate was changed to leflunomide at a daily dose of 20 mg due to its ineffectiveness for arthritis at the end of 2011. As RA remained active with a high Disease Activity Score-28 (DAS-28) index, reaching up to 5.43, leflunomide was stopped, and an inhibitor of tumour necrosis factor-alpha etanercept at 50 mg per week, was prescribed in 2013 and continued for 10 years. During this treatment, low disease activity of RA was maintained with short-term exacerbations, and no significant side effects were observed. The DAS-28 index ranged from 1.32 to 3.47. However, AA persisted throughout this period without significant improvement or deterioration. An exacerbation of RA and AA was noticed at the beginning of 2023, leading to the decision to stop etanercept and to start therapy with the selective Janus kinase (JAK) 1 inhibitor upadacitinib at a dose of 15 mg daily. Upadacitinib was prescribed as it was the only JAK inhibitor reimbursed in Lithuania at that time. During the visit, trichoscopy of the scalp was performed and showed broken hairs, black and yellow dots, vellus hairs, with a Severity of Alopecia Tool (SALT) score of 51 (Figure 1a). A significant improvement in RA was observed within 3 months, with the DAS-28 decreasing from 2.21 to 1.18. The hair regrew completely after 6 months with the SALT score of 0 and with no evidence of disease activity on trichoscopy (Figure 1b,c). No side effects were observed with upadacitinib, and laboratory tests performed every 3 months returned normal results.
AA is associated with autoimmune diseases such as RA due to the similar involvement of the JAK and signal transducer and activator of transcription signalling pathway (JAK/STAT).1, 2 Cytokines such interferon-γ, interleukin-2 (IL-2), interleukin-7 (IL-7) and interleukin-15 (IL-15) are believed to play an important role in the pathogenesis of AA. These cytokines activate certain JAK molecules, leading to the phosphorylation of the corresponding domains of the STAT pathway. This phosphorylation ultimately leads to the transcription of the target gene.3 JAK inhibitors hold promise as a new treatment for AA. In June 2022, the Food and Drug Administration (FDA) authorised baricitinib for the treatment of severe AA and in June 2023, the FDA approved another JAK inhibitor, called ritlecitinib.4 However, upadacitinib and ruxolitinib have not yet been approved for the treatment of AA. Upadacitinib is a selective JAK-1 inhibitor, which blocks signalling of many inflammatory cytokines, including IL-2, IL-6, IL-7 and IL-15, suppressing the inflammation common to both diseases.5, 6 Several successful cases of upadacitinib 15 or 20 mg daily in patients with AA and concomitant atopic dermatitis or Crohn's disease have been published in the literature.7, 8 In this letter, we provide evidence that upadacitinib at 15 mg daily could be an effective treatment for AA in patients with RA.
Ieva Lingytė: Conception of the work; Data analysis and interpretation, Drafting the article. Paula Kaminskienė: Data analysis and interpretation, Drafting the article. Arūnas Petkevičius: Critical revision of the article, Final approval of the version to be published. Asta Baranauskaitė: Conception of the work; Data collection; Critical revision of the article; Final approval of the version to be published.
The authors declare no conflict of interest.
All patients in this manuscript have given written informed consent for participation in the study and the use of their deidentified, anonymized, aggregated data and their case details (including photographs) for publication. Ethical Approval: not applicable.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
