Tarek Ajami, Sunwoo Han, Ruben Blachman-Braun, Helen Y. Hougen, Yuval Avda, Mark L. Gonzalgo, Bruno Nahar, Sanoj Punnen, Dipen J. Parekh, Isildinha M. Reis, Chad R. Ritch
{"title":"Optimal Management for Primary High Grade Ta Bladder Cancer: Role of re-staging TURBT and Intravesical Adjuvant Therapy","authors":"Tarek Ajami, Sunwoo Han, Ruben Blachman-Braun, Helen Y. Hougen, Yuval Avda, Mark L. Gonzalgo, Bruno Nahar, Sanoj Punnen, Dipen J. Parekh, Isildinha M. Reis, Chad R. Ritch","doi":"10.1002/bco2.363","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>This study aims to investigate the impact of risk group classification, restaging transurethral resection (re-TURBT), and adjuvant treatment intensity on recurrence and progression risks in high-grade Ta tumours in patients with non-muscle invasive bladder cancer (NMIBC).</p>\n </section>\n \n <section>\n \n <h3> Materials and methods</h3>\n \n <p>Data from a comprehensive bladder cancer database were utilized for this study. Patients with primary high-grade Ta tumours were included. Risk groups were classified according to AUA/SUO criteria. Tumour characteristics and patient demographics were analysed using descriptive statistics. Cox proportional hazard regression models were used to assess the effect of re-TURBT and other clinical/treatment-related predictors on recurrence- and progression-free survivals. The survivals by selected predictors were estimated using Kaplan–Meier method, and groups were compared by the log-rank test.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Among 218 patients with high-grade Ta bladder cancer, those who underwent re-TURBT had significantly better 5-year recurrence-free survival (71.1% vs. 26.8%, <i>p</i> = 0.0009) and progression-free survival (98.6% vs. 73%, <i>p</i> = 0.0018) compared with those with initial TURBT alone. Full BCG treatment (induction and maintenance) showed lower recurrence risk, especially in high-risk patients. However, residual disease at re-TURBT did not significantly affect recurrence risk.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>This study highlights the significance of risk group classification, the role of re-TURBT, and the intensity of adjuvant treatment in the management of high-grade Ta tumours. A risk-adapted model is crucial to reduce the burden of unnecessary intravesical treatment and endoscopic procedures.</p>\n </section>\n </div>","PeriodicalId":72420,"journal":{"name":"BJUI compass","volume":"5 8","pages":"913-919"},"PeriodicalIF":1.9000,"publicationDate":"2024-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/bco2.363","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJUI compass","FirstCategoryId":"1085","ListUrlMain":"https://bjui-journals.onlinelibrary.wiley.com/doi/10.1002/bco2.363","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
This study aims to investigate the impact of risk group classification, restaging transurethral resection (re-TURBT), and adjuvant treatment intensity on recurrence and progression risks in high-grade Ta tumours in patients with non-muscle invasive bladder cancer (NMIBC).
Materials and methods
Data from a comprehensive bladder cancer database were utilized for this study. Patients with primary high-grade Ta tumours were included. Risk groups were classified according to AUA/SUO criteria. Tumour characteristics and patient demographics were analysed using descriptive statistics. Cox proportional hazard regression models were used to assess the effect of re-TURBT and other clinical/treatment-related predictors on recurrence- and progression-free survivals. The survivals by selected predictors were estimated using Kaplan–Meier method, and groups were compared by the log-rank test.
Results
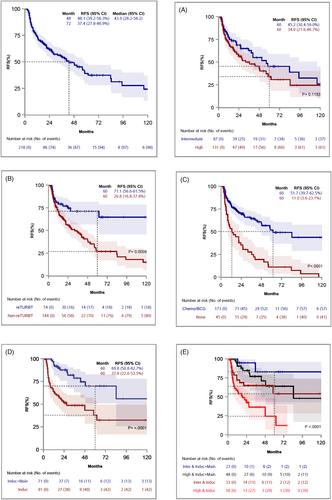
Among 218 patients with high-grade Ta bladder cancer, those who underwent re-TURBT had significantly better 5-year recurrence-free survival (71.1% vs. 26.8%, p = 0.0009) and progression-free survival (98.6% vs. 73%, p = 0.0018) compared with those with initial TURBT alone. Full BCG treatment (induction and maintenance) showed lower recurrence risk, especially in high-risk patients. However, residual disease at re-TURBT did not significantly affect recurrence risk.
Conclusions
This study highlights the significance of risk group classification, the role of re-TURBT, and the intensity of adjuvant treatment in the management of high-grade Ta tumours. A risk-adapted model is crucial to reduce the burden of unnecessary intravesical treatment and endoscopic procedures.
本研究旨在探讨非肌层浸润性膀胱癌(NMIBC)患者中,危险组别分类、重新分期经尿道切除术(re-TURBT)和辅助治疗强度对高级别Ta肿瘤复发和进展风险的影响。本研究利用了综合膀胱癌数据库中的数据,纳入了原发性高级别Ta肿瘤患者。根据AUA/SUO标准划分了风险组别。采用描述性统计对肿瘤特征和患者人口统计学特征进行了分析。Cox比例危险回归模型用于评估再次TURBT和其他临床/治疗相关预测因素对复发和无进展生存率的影响。在218例高级别Ta膀胱癌患者中,与单纯初次TURBT相比,接受再次TURBT的患者5年无复发生存率(71.1% vs. 26.8%,p = 0.0009)和无进展生存率(98.6% vs. 73%,p = 0.0018)明显更高。全面卡介苗治疗(诱导和维持)降低了复发风险,尤其是在高危患者中。这项研究强调了风险组别分类、再TURBT的作用以及辅助治疗的强度在治疗高级别Ta肿瘤中的重要性。风险适应模型对于减少不必要的膀胱内治疗和内镜手术负担至关重要。



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
