Health equity in clinical trials for regional, rural and First nations communities: Need for networked clinical trial system, through a values and purpose-aligned system culture
{"title":"Health equity in clinical trials for regional, rural and First nations communities: Need for networked clinical trial system, through a values and purpose-aligned system culture","authors":"Sabe Sabesan FRACP, Melanie Poxton B Nursing","doi":"10.1111/ajr.13122","DOIUrl":null,"url":null,"abstract":"<p>Clinical trials are essential components of health practice and are vital to developing new therapies, advancing interventions, improving service delivery and enhancing models of care.<span><sup>1</sup></span> For patients, participation in clinical trials improves outcomes in many disease areas and reduces variation in practice, due to strict monitoring requirements. For health practitioners, clinical trials present an opportunity to be at the cutting edge of best practice. For services, clinical trials improve standard procedures. For health systems, industry sponsored trials are an additional source of revenue that could be reinvested to build clinical trial units. Reports suggest that there is significant return on investment in this sector.<span><sup>2</sup></span></p><p>For these and other reasons, the new National Clinical Trial Governance Framework has called for clinical trials to be included as a routine aspect of clinical practice.<span><sup>3</sup></span> In the cancer care sector, which serves a significant number of patients with incurable diseases, international guidelines recommend clinical trials as the first option.<span><sup>4</sup></span> This means, to be aligned with international best practice, every cancer service should be offering clinical trials to all cancer patients regardless of postcode, at least for patients with incurable diseases.</p><p>Australia and many Western countries have invested significant resources to build clinical trial capabilities and enable engagement in local and international trials. However, people in regional, rural and First nations communities continue to have limited access to trials close to home.<span><sup>5, 6</sup></span> As a result, they must endure substantial travel, major costs and inconvenience, and often, must relocate to metropolitan centres or pass up the opportunity to participate. This is a key challenge highlighted by the accompanying commentary (Walsh et al.)<span><sup>7</sup></span> and specifically emphasised in the accompanying research paper (McPhee et al.).<span><sup>7, 8</sup></span> Alarmingly, an MJA study recently described particularly poor representation of First nations communities in trials (exemplified in trials of parenting programs).<span><sup>9</sup></span></p><p>Many of the challenges and barriers to health services in regional, rural and First nations communities are apparent (or even more pronounced) in the case of clinical trials. Workforce shortages and turn over at all levels, limited skills and awareness among staff of the potential benefit of trials, and inadequate investment in infrastructure are common. This constrains such sites from attracting sponsors and hosting clinical trials as stand-alone sites. Beyond this, system cultural issues within rural and First nations services may stifle participation, or the economic imperatives of metropolitan trial units and their sponsors may overrule.</p><p>In the light of the above, it is not unreasonable to conclude that the majority of regional, rural, remote and First nations health services are unable to function as stand-alone sites for clinical trials. As an alternative, a networked approach that decentralises trial access has been advocated by Government reviews and Government strategic plans, including by bodies such as the NH&MRC. It is pleasing to see a commentary recommending such decentralised trials in this edition (Walsh et al.).<span><sup>7</sup></span> As an example, to establish decentralised clinical trials at system level, the Commonwealth Government, via the Medical Research Future Fund (MRFF), have funded states and territories to establish the Australian Teletrial Program led by Queensland health, likewise, the New South Wales and Australian Capital Territory governments established regional, rural and remote trial programs in 2019.</p><p>These two initiatives, with combined value of $100 M, use the Australasian Teletrial Model (originally designed by the rural and regional group of Clinical Oncology Society of Australia) as the mechanism to connect larger and smaller sites to form trial clusters. In that way, some or all aspects of trials can potentially be offered at smaller centres across the country. (Operational details of this model can be found in the National Teletrials Compendium; https://www.health.gov.au/resources/collections/the-national-teletrials-compendium).</p><p>These programs aspire to set up an enabling infrastructure, establish regulatory processes and build capacity to create a viable networked and decentralised trial system. Likewise, the PARTNER program aims to build trial capacity in regional and rural primary care practices (https://partnernetwork.com.au/). Such programs use regional clinical trial coordinating centres (RCCC) in each state/territory to help clinicians navigate the necessary approval processes. Over the last 2 years, some trials have been conducted via the teletrial model. This has improved patient access to trials across rural, regional and remote sites across many diseases.</p><p>We now have a $100 M program to improve trial access to regional, rural, remote and First nations communities. Health services in all states and territories are incorporating trials into their strategic plans. This enabling infrastructure program relies on overarching system ownership, engagement and leadership across all layers of the national, state and territory heath systems. It will require a values and purpose aligned system culture, which can support and enable program officers, RCCC staff and champions departments of health, health services and the frontline workforce, to drive uptake at clinical levels.</p><p>The current culture of health services working in isolation in Australia does not provide the platform for collaboration and impedes harmonised national regulatory processes, resulting in long and variable regulatory work for trial coordinators, clinical researchers and sponsors. Working as clinicians in Townsville, designing, piloting and publishing on telehealth programs to provide care closer to home, the lack of alignment across systems and strategic plans is frustrating and has become a major psychological hazard for everyone involved. However, for patients, it is fundamentally a question of poor health equity and not having access to life changing and saving therapy.</p><p>This is one of the reasons the Clinical Oncology Society of Australia (COSA) and its national partners have embarked on an advocacy program for workplace culture reforms and have called for a new narrative on healthy workplace culture.<span><sup>10</sup></span> COSA proposes a well-being centred definition and a System Lasagne model for creating healthy workplace cultures in democratic societies such as ours. A more values and purpose aligned culture is likely to ensure a greater focus on health equity, which in turn may ensure that programs related to regional, rural, remote and First nations communities will be better embedded into the whole of the system as illustrated in Figure 1.</p><p>Together we do better, putting our people and communities first through action. Indeed, when we create a more values and purpose aligned health system culture, we will also be able to see clinical trials, teletrials and best practice initiatives more seamlessly embedded into systems and managed as core business. When the workforce is inspired by such systems, they are likely to be engaged and productive in their workplaces and remain mentally and physically well.</p><p><b>Sabe Sabesan:</b> Conceptualization; methodology; formal analysis; data curation; writing – original draft; writing – review and editing; project administration; validation. <b>Melanie Poxton:</b> Conceptualization; writing – review and editing; methodology; data curation; validation.</p><p>Two authors declare no conflict of interest.</p>","PeriodicalId":55421,"journal":{"name":"Australian Journal of Rural Health","volume":"32 3","pages":"588-591"},"PeriodicalIF":2.1000,"publicationDate":"2024-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ajr.13122","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Australian Journal of Rural Health","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ajr.13122","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"NURSING","Score":null,"Total":0}
引用次数: 0
Abstract
Clinical trials are essential components of health practice and are vital to developing new therapies, advancing interventions, improving service delivery and enhancing models of care.1 For patients, participation in clinical trials improves outcomes in many disease areas and reduces variation in practice, due to strict monitoring requirements. For health practitioners, clinical trials present an opportunity to be at the cutting edge of best practice. For services, clinical trials improve standard procedures. For health systems, industry sponsored trials are an additional source of revenue that could be reinvested to build clinical trial units. Reports suggest that there is significant return on investment in this sector.2
For these and other reasons, the new National Clinical Trial Governance Framework has called for clinical trials to be included as a routine aspect of clinical practice.3 In the cancer care sector, which serves a significant number of patients with incurable diseases, international guidelines recommend clinical trials as the first option.4 This means, to be aligned with international best practice, every cancer service should be offering clinical trials to all cancer patients regardless of postcode, at least for patients with incurable diseases.
Australia and many Western countries have invested significant resources to build clinical trial capabilities and enable engagement in local and international trials. However, people in regional, rural and First nations communities continue to have limited access to trials close to home.5, 6 As a result, they must endure substantial travel, major costs and inconvenience, and often, must relocate to metropolitan centres or pass up the opportunity to participate. This is a key challenge highlighted by the accompanying commentary (Walsh et al.)7 and specifically emphasised in the accompanying research paper (McPhee et al.).7, 8 Alarmingly, an MJA study recently described particularly poor representation of First nations communities in trials (exemplified in trials of parenting programs).9
Many of the challenges and barriers to health services in regional, rural and First nations communities are apparent (or even more pronounced) in the case of clinical trials. Workforce shortages and turn over at all levels, limited skills and awareness among staff of the potential benefit of trials, and inadequate investment in infrastructure are common. This constrains such sites from attracting sponsors and hosting clinical trials as stand-alone sites. Beyond this, system cultural issues within rural and First nations services may stifle participation, or the economic imperatives of metropolitan trial units and their sponsors may overrule.
In the light of the above, it is not unreasonable to conclude that the majority of regional, rural, remote and First nations health services are unable to function as stand-alone sites for clinical trials. As an alternative, a networked approach that decentralises trial access has been advocated by Government reviews and Government strategic plans, including by bodies such as the NH&MRC. It is pleasing to see a commentary recommending such decentralised trials in this edition (Walsh et al.).7 As an example, to establish decentralised clinical trials at system level, the Commonwealth Government, via the Medical Research Future Fund (MRFF), have funded states and territories to establish the Australian Teletrial Program led by Queensland health, likewise, the New South Wales and Australian Capital Territory governments established regional, rural and remote trial programs in 2019.
These two initiatives, with combined value of $100 M, use the Australasian Teletrial Model (originally designed by the rural and regional group of Clinical Oncology Society of Australia) as the mechanism to connect larger and smaller sites to form trial clusters. In that way, some or all aspects of trials can potentially be offered at smaller centres across the country. (Operational details of this model can be found in the National Teletrials Compendium; https://www.health.gov.au/resources/collections/the-national-teletrials-compendium).
These programs aspire to set up an enabling infrastructure, establish regulatory processes and build capacity to create a viable networked and decentralised trial system. Likewise, the PARTNER program aims to build trial capacity in regional and rural primary care practices (https://partnernetwork.com.au/). Such programs use regional clinical trial coordinating centres (RCCC) in each state/territory to help clinicians navigate the necessary approval processes. Over the last 2 years, some trials have been conducted via the teletrial model. This has improved patient access to trials across rural, regional and remote sites across many diseases.
We now have a $100 M program to improve trial access to regional, rural, remote and First nations communities. Health services in all states and territories are incorporating trials into their strategic plans. This enabling infrastructure program relies on overarching system ownership, engagement and leadership across all layers of the national, state and territory heath systems. It will require a values and purpose aligned system culture, which can support and enable program officers, RCCC staff and champions departments of health, health services and the frontline workforce, to drive uptake at clinical levels.
The current culture of health services working in isolation in Australia does not provide the platform for collaboration and impedes harmonised national regulatory processes, resulting in long and variable regulatory work for trial coordinators, clinical researchers and sponsors. Working as clinicians in Townsville, designing, piloting and publishing on telehealth programs to provide care closer to home, the lack of alignment across systems and strategic plans is frustrating and has become a major psychological hazard for everyone involved. However, for patients, it is fundamentally a question of poor health equity and not having access to life changing and saving therapy.
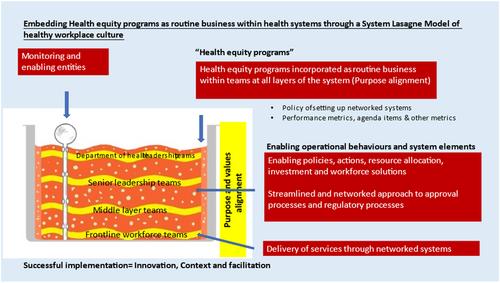
This is one of the reasons the Clinical Oncology Society of Australia (COSA) and its national partners have embarked on an advocacy program for workplace culture reforms and have called for a new narrative on healthy workplace culture.10 COSA proposes a well-being centred definition and a System Lasagne model for creating healthy workplace cultures in democratic societies such as ours. A more values and purpose aligned culture is likely to ensure a greater focus on health equity, which in turn may ensure that programs related to regional, rural, remote and First nations communities will be better embedded into the whole of the system as illustrated in Figure 1.
Together we do better, putting our people and communities first through action. Indeed, when we create a more values and purpose aligned health system culture, we will also be able to see clinical trials, teletrials and best practice initiatives more seamlessly embedded into systems and managed as core business. When the workforce is inspired by such systems, they are likely to be engaged and productive in their workplaces and remain mentally and physically well.
Sabe Sabesan: Conceptualization; methodology; formal analysis; data curation; writing – original draft; writing – review and editing; project administration; validation. Melanie Poxton: Conceptualization; writing – review and editing; methodology; data curation; validation.
期刊介绍:
The Australian Journal of Rural Health publishes articles in the field of rural health. It facilitates the formation of interdisciplinary networks, so that rural health professionals can form a cohesive group and work together for the advancement of rural practice, in all health disciplines. The Journal aims to establish a national and international reputation for the quality of its scholarly discourse and its value to rural health professionals. All articles, unless otherwise identified, are peer reviewed by at least two researchers expert in the field of the submitted paper.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
