Patients with complete clinical response after neoadjuvant chemoradiotherapy for locally advanced esophageal cancer: A Markov decision analysis of esophagectomy versus active surveillance
Adom Bondzi-Simpson MD, MSc , Tiago Ribeiro MD , Angelo Grant BHSc , Michael Ko MD, PhD , Natalie Coburn MD, MPH , Julie Hallet MD, MSc , Girish S. Kulkarni MD, PhD , Biniam Kidane MD, MSc
{"title":"Patients with complete clinical response after neoadjuvant chemoradiotherapy for locally advanced esophageal cancer: A Markov decision analysis of esophagectomy versus active surveillance","authors":"Adom Bondzi-Simpson MD, MSc , Tiago Ribeiro MD , Angelo Grant BHSc , Michael Ko MD, PhD , Natalie Coburn MD, MPH , Julie Hallet MD, MSc , Girish S. Kulkarni MD, PhD , Biniam Kidane MD, MSc","doi":"10.1016/j.jtcvs.2024.04.020","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div><span>Chemoradiation<span> followed by esophagectomy is a standard treatment option for patients with locally advanced </span></span>esophageal cancer (LAEC). Esophagectomy is a high-risk procedure, and recent evidence suggests select patients may benefit from omitting or delaying surgery. This study aims to compare surgery versus active surveillance for LAEC patients with complete clinical response (cCR) after neoadjuvant chemoradiotherapy (nCRT).</div></div><div><h3>Methods</h3><div>Decision analysis with Markov modeling was used. The base case was a 60-year-old man with T3N0M0 esophageal cancer with cCR after nCRT. The decision was modeled for a 5-year time horizon. Primary outcomes were life-years and quality-adjusted life-years (QALY). Probabilities and utilities were derived through the literature. Deterministic sensitivity analyses were performed using ranges from the literature with consideration for clinical plausibility.</div></div><div><h3>Results</h3><div>Surgery was favored for survival with an expected life-years of 2.89 versus 2.64. After incorporating quality of life, active surveillance was favored, with an expected QALY of 1.70 versus 1.56. The model was sensitive to probability of recurrence on active surveillance (threshold value 0.598), probability of recurrence being resectable (0.318), and disutility of previous esophagectomy (−0.091). The model was not sensitive to perioperative morbidity and mortality.</div></div><div><h3>Conclusions</h3><div>Our study finds that surgery increases life expectancy but decreases QALY. Although the incremental change in QALY for either modality is insufficient to make broad clinical recommendations, our study demonstrates that either approach is acceptable. As probabilities of key factors are further defined in the literature, treatment decisions for patients with LAEC and a cCR after nCRT should consider histology, patient values, and quality of life.</div></div>","PeriodicalId":49975,"journal":{"name":"Journal of Thoracic and Cardiovascular Surgery","volume":"168 6","pages":"Pages 1538-1549.e1"},"PeriodicalIF":4.4000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0022522324003647","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
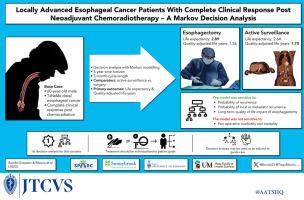
Chemoradiation followed by esophagectomy is a standard treatment option for patients with locally advanced esophageal cancer (LAEC). Esophagectomy is a high-risk procedure, and recent evidence suggests select patients may benefit from omitting or delaying surgery. This study aims to compare surgery versus active surveillance for LAEC patients with complete clinical response (cCR) after neoadjuvant chemoradiotherapy (nCRT).
Methods
Decision analysis with Markov modeling was used. The base case was a 60-year-old man with T3N0M0 esophageal cancer with cCR after nCRT. The decision was modeled for a 5-year time horizon. Primary outcomes were life-years and quality-adjusted life-years (QALY). Probabilities and utilities were derived through the literature. Deterministic sensitivity analyses were performed using ranges from the literature with consideration for clinical plausibility.
Results
Surgery was favored for survival with an expected life-years of 2.89 versus 2.64. After incorporating quality of life, active surveillance was favored, with an expected QALY of 1.70 versus 1.56. The model was sensitive to probability of recurrence on active surveillance (threshold value 0.598), probability of recurrence being resectable (0.318), and disutility of previous esophagectomy (−0.091). The model was not sensitive to perioperative morbidity and mortality.
Conclusions
Our study finds that surgery increases life expectancy but decreases QALY. Although the incremental change in QALY for either modality is insufficient to make broad clinical recommendations, our study demonstrates that either approach is acceptable. As probabilities of key factors are further defined in the literature, treatment decisions for patients with LAEC and a cCR after nCRT should consider histology, patient values, and quality of life.
期刊介绍:
The Journal of Thoracic and Cardiovascular Surgery presents original, peer-reviewed articles on diseases of the heart, great vessels, lungs and thorax with emphasis on surgical interventions. An official publication of The American Association for Thoracic Surgery and The Western Thoracic Surgical Association, the Journal focuses on techniques and developments in acquired cardiac surgery, congenital cardiac repair, thoracic procedures, heart and lung transplantation, mechanical circulatory support and other procedures.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
