{"title":"Radiofrecuencia del nervio supraescapular como estrategia analgésica para el dolor crónico de hombro. Revisión sistemática y metaanálisis","authors":"","doi":"10.1016/j.redar.2024.03.004","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><div>Chronic shoulder pain is highly prevalent in the general population. Many different analgesic strategies have been described, including radiofrequency treatment to the suprascapular nerve (RFS); however, the effectiveness this approach remains unclear, and no strong recommendation can be made. The aim of this systematic review is to analyse the latest clinical trials evaluating the effectiveness of RFS techniques applied to the suprascapular nerve in terms of management of chronic shoulder pain, post-procedural functionality, and adverse effects.</div></div><div><h3>Methods</h3><div>We performed a systematic review of clinical trials retrieved from Medline, Embase and the cCentral databases. We included trials comparing RFS with other strategies, including placebo, that had as their primary outcome measures pain rated on a visual analogue scale, functionality rated on a shoulder pain and disability index (SPADI), and the incidence of adverse events. Risk of bias was analysed using the Cochrane RoB2 tool. Evidence was analysed using a random effects model and heterogeneity was quantified using the I<sup>2</sup> test.</div></div><div><h3>Results</h3><div>We identified 3030 trials, of which 8 met the inclusion criteria (n<!--> <!-->=<!--> <!-->408). Seven had a high risk of bias. Pain intensity at 1 and 3 months was lower in patients receiving RFS, with a standardised mean difference (SMD) of −0.9 (95% CI: −1.1-0.33; <em>P</em>=.29; I<sup>2</sup> 88%; <em>P</em><.001) and −1.17 (95% CI: −2.49-0.14; <em>P</em>=.08; I<sup>2</sup> 97%; <em>P</em><.001), respectively. Functional compromise at 1 and 3 months decreased in patients receiving RFS, with an SMD of -0.31 (95% CI: −0.91-0.29; <em>P</em>=.31; I<sup>2</sup> 80%; <em>P</em><.001) and −1.54 (95% CI: −3.26-0.19; <em>P</em>=.08; I<sup>2</sup> 98%; <em>P</em><.001), respectively. No RFS-related adverse events were described.</div></div><div><h3>Conclusion</h3><div>The evidence suggests that RFS reduces pain and improves functionality. However, the certainty of the evidence is low.</div></div>","PeriodicalId":46479,"journal":{"name":"Revista Espanola de Anestesiologia y Reanimacion","volume":"71 9","pages":"Pages 678-686"},"PeriodicalIF":0.8000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista Espanola de Anestesiologia y Reanimacion","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0034935624000744","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
Chronic shoulder pain is highly prevalent in the general population. Many different analgesic strategies have been described, including radiofrequency treatment to the suprascapular nerve (RFS); however, the effectiveness this approach remains unclear, and no strong recommendation can be made. The aim of this systematic review is to analyse the latest clinical trials evaluating the effectiveness of RFS techniques applied to the suprascapular nerve in terms of management of chronic shoulder pain, post-procedural functionality, and adverse effects.
Methods
We performed a systematic review of clinical trials retrieved from Medline, Embase and the cCentral databases. We included trials comparing RFS with other strategies, including placebo, that had as their primary outcome measures pain rated on a visual analogue scale, functionality rated on a shoulder pain and disability index (SPADI), and the incidence of adverse events. Risk of bias was analysed using the Cochrane RoB2 tool. Evidence was analysed using a random effects model and heterogeneity was quantified using the I2 test.
Results
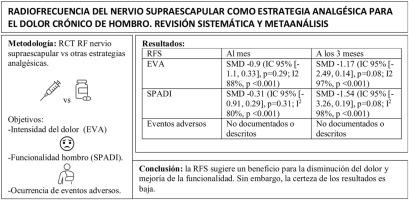
We identified 3030 trials, of which 8 met the inclusion criteria (n = 408). Seven had a high risk of bias. Pain intensity at 1 and 3 months was lower in patients receiving RFS, with a standardised mean difference (SMD) of −0.9 (95% CI: −1.1-0.33; P=.29; I2 88%; P<.001) and −1.17 (95% CI: −2.49-0.14; P=.08; I2 97%; P<.001), respectively. Functional compromise at 1 and 3 months decreased in patients receiving RFS, with an SMD of -0.31 (95% CI: −0.91-0.29; P=.31; I2 80%; P<.001) and −1.54 (95% CI: −3.26-0.19; P=.08; I2 98%; P<.001), respectively. No RFS-related adverse events were described.
Conclusion
The evidence suggests that RFS reduces pain and improves functionality. However, the certainty of the evidence is low.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
