{"title":"National trends, safety, and effectiveness of minimally invasive concomitant chest wall resection for locally advanced lung cancer","authors":"Shawn Purnell MD , Ayham Odeh MD , Richard Freeman MD, MBA , Wissam Raad MD, FACS , Elliot Servais MD, FACS , Zaid Abdelsattar MD, MS, FACS","doi":"10.1016/j.xjon.2024.03.016","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>Concomitant chest wall resection for locally advanced lung cancer is traditionally performed via an open approach. The safety and effectiveness of minimally invasive approaches for chest wall resections are unknown.</p></div><div><h3>Methods</h3><p>We used the National Cancer Database to identify patients undergoing lobectomy/bi-lobectomy with concomitant chest wall resection from 2010 to 2020. We stratified patients into those undergoing a minimally invasive resection (video-assisted thoracoscopic surgery [VATS]/robotic) or open, while accounting for conversions. We also compared VATS with robotic approaches. The main outcomes were length of stay, mortality, readmissions, and overall survival. We used multivariable, Kaplan-Meier and Cox proportional models to identify associations.</p></div><div><h3>Results</h3><p>Of 2837 patients, 756 procedures (26.6%) were started minimally invasive, of which 23.1% were robotic. There were 237 (31.3%) conversions. Patients undergoing a minimally invasive operation were similar in terms of age (65.2 ± 9.8 years vs 66.0 ± 9.9 years), sex, race, tumor histology, and location (all <em>P</em> > .05) but had smaller cancers (5.4 ± 2.6 cm vs 6.2 ± 4.3 cm; <em>P</em> < .001) compared with those undergoing open. They also had shorter length of stay (8.6 ± 7.6 days vs 9.7 ± 9.3 days; <em>P</em> < .001) but similar unadjusted 90-day mortality (8.2% vs 8.0%; <em>P</em> = .999). Neoadjuvant therapy was associated with less minimally invasive approaches (adjusted odds ratio, 0.69; <em>P</em> ≤ .001). Larger cancers were associated with less minimally invasive operations and greater rates of conversions. However, the robotic approach was associated with lower conversion rates than VATS across all tumor sizes. Overall survival was equivalent.</p></div><div><h3>Conclusions</h3><p>The use of minimally invasive approaches to concomitant chest wall resection is increasing. Although conversions to open are common, this approach is safe and is associated with shorter hospital stays. Overall survival is equivalent to the open approach.</p></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":"19 ","pages":"Pages 311-324"},"PeriodicalIF":1.9000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2666273624000974/pdfft?md5=23e283284243639c052996ec280658de&pid=1-s2.0-S2666273624000974-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273624000974","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/6 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
Concomitant chest wall resection for locally advanced lung cancer is traditionally performed via an open approach. The safety and effectiveness of minimally invasive approaches for chest wall resections are unknown.
Methods
We used the National Cancer Database to identify patients undergoing lobectomy/bi-lobectomy with concomitant chest wall resection from 2010 to 2020. We stratified patients into those undergoing a minimally invasive resection (video-assisted thoracoscopic surgery [VATS]/robotic) or open, while accounting for conversions. We also compared VATS with robotic approaches. The main outcomes were length of stay, mortality, readmissions, and overall survival. We used multivariable, Kaplan-Meier and Cox proportional models to identify associations.
Results
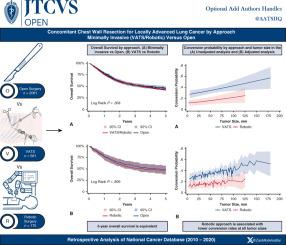
Of 2837 patients, 756 procedures (26.6%) were started minimally invasive, of which 23.1% were robotic. There were 237 (31.3%) conversions. Patients undergoing a minimally invasive operation were similar in terms of age (65.2 ± 9.8 years vs 66.0 ± 9.9 years), sex, race, tumor histology, and location (all P > .05) but had smaller cancers (5.4 ± 2.6 cm vs 6.2 ± 4.3 cm; P < .001) compared with those undergoing open. They also had shorter length of stay (8.6 ± 7.6 days vs 9.7 ± 9.3 days; P < .001) but similar unadjusted 90-day mortality (8.2% vs 8.0%; P = .999). Neoadjuvant therapy was associated with less minimally invasive approaches (adjusted odds ratio, 0.69; P ≤ .001). Larger cancers were associated with less minimally invasive operations and greater rates of conversions. However, the robotic approach was associated with lower conversion rates than VATS across all tumor sizes. Overall survival was equivalent.
Conclusions
The use of minimally invasive approaches to concomitant chest wall resection is increasing. Although conversions to open are common, this approach is safe and is associated with shorter hospital stays. Overall survival is equivalent to the open approach.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
