Maximilian A. Fliegner BA , Hechuan Hou MS , Tyler M. Bauer MD , Temilolaoluwa Daramola MD , Jeffrey S. McCullough PhD , Francis D. Pagani MD, PhD , Devraj Sukul MD, MSc , Donald S. Likosky PhD , Steven J. Keteyian PhD , Michael P. Thompson PhD
{"title":"Interhospital variability in cardiac rehabilitation use after cardiac surgery among Medicare beneficiaries","authors":"Maximilian A. Fliegner BA , Hechuan Hou MS , Tyler M. Bauer MD , Temilolaoluwa Daramola MD , Jeffrey S. McCullough PhD , Francis D. Pagani MD, PhD , Devraj Sukul MD, MSc , Donald S. Likosky PhD , Steven J. Keteyian PhD , Michael P. Thompson PhD","doi":"10.1016/j.jtcvs.2024.04.019","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>Despite guideline recommendation, cardiac rehabilitation (CR) after cardiac surgery remains underused, and the extent of interhospital variability is not well understood. This study evaluated determinants of interhospital variability in CR use and outcomes.</div></div><div><h3>Methods</h3><div>This retrospective cohort study included 166,809 Medicare beneficiaries undergoing cardiac surgery who were discharged alive between July 1, 2016, and December 31, 2018. CR participation was identified in outpatient facility claims within a year of discharge. Hospital-level CR rates were tabulated, and multilevel models evaluated the extent to which patient, organizational, and regional factors accounted for interhospital variability. Adjusted 1-year mortality and readmission rates were also calculated for each hospital quartile of CR use.</div></div><div><h3>Results</h3><div><span>Overall, 90,171 (54.1%) participated in at least 1 CR session within a year of discharge. Interhospital CR rates ranged from 0.0% to 96.8%. Hospital factors that predicted CR use included nonteaching status and lower-hospital volume. Before adjustment for patient, organizational, and regional factors, 19.3% of interhospital variability was attributable to the admitting hospital. After accounting for covariates, 12.3% of variation was attributable to the admitting hospital. Patient (0.5%), structural (2.8%), and regional (3.7%) factors accounted for the remaining explained variation. Hospitals in the lowest quartile of CR use had greater adjusted 1-year mortality rates (Q1 = 6.7%, Q4 = 5.2%, </span><em>P</em> < .001) and readmission rates (Q1 = 37.6%, Q4 = 33.9%, <em>P</em> < .001).</div></div><div><h3>Conclusions</h3><div>Identifying best practices among high CR use facilities and barriers to access in low CR use hospitals may reduce interhospital variability in CR use and advance national improvement efforts.</div></div>","PeriodicalId":49975,"journal":{"name":"Journal of Thoracic and Cardiovascular Surgery","volume":"169 3","pages":"Pages 916-923.e5"},"PeriodicalIF":4.4000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0022522324003635","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/20 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
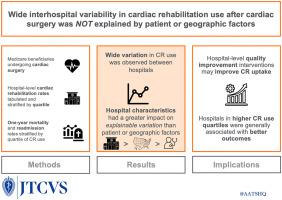
Despite guideline recommendation, cardiac rehabilitation (CR) after cardiac surgery remains underused, and the extent of interhospital variability is not well understood. This study evaluated determinants of interhospital variability in CR use and outcomes.
Methods
This retrospective cohort study included 166,809 Medicare beneficiaries undergoing cardiac surgery who were discharged alive between July 1, 2016, and December 31, 2018. CR participation was identified in outpatient facility claims within a year of discharge. Hospital-level CR rates were tabulated, and multilevel models evaluated the extent to which patient, organizational, and regional factors accounted for interhospital variability. Adjusted 1-year mortality and readmission rates were also calculated for each hospital quartile of CR use.
Results
Overall, 90,171 (54.1%) participated in at least 1 CR session within a year of discharge. Interhospital CR rates ranged from 0.0% to 96.8%. Hospital factors that predicted CR use included nonteaching status and lower-hospital volume. Before adjustment for patient, organizational, and regional factors, 19.3% of interhospital variability was attributable to the admitting hospital. After accounting for covariates, 12.3% of variation was attributable to the admitting hospital. Patient (0.5%), structural (2.8%), and regional (3.7%) factors accounted for the remaining explained variation. Hospitals in the lowest quartile of CR use had greater adjusted 1-year mortality rates (Q1 = 6.7%, Q4 = 5.2%, P < .001) and readmission rates (Q1 = 37.6%, Q4 = 33.9%, P < .001).
Conclusions
Identifying best practices among high CR use facilities and barriers to access in low CR use hospitals may reduce interhospital variability in CR use and advance national improvement efforts.
期刊介绍:
The Journal of Thoracic and Cardiovascular Surgery presents original, peer-reviewed articles on diseases of the heart, great vessels, lungs and thorax with emphasis on surgical interventions. An official publication of The American Association for Thoracic Surgery and The Western Thoracic Surgical Association, the Journal focuses on techniques and developments in acquired cardiac surgery, congenital cardiac repair, thoracic procedures, heart and lung transplantation, mechanical circulatory support and other procedures.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
