Prediction of Individual Disease Progression Including Parameter Uncertainty in Rare Neurodegenerative Diseases: The Example of Autosomal-Recessive Spastic Ataxia Charlevoix Saguenay (ARSACS)
Niels Hendrickx, France Mentré, Andreas Traschütz, Cynthia Gagnon, Rebecca Schüle, Matthis Synofzik, Emmanuelle Comets
{"title":"Prediction of Individual Disease Progression Including Parameter Uncertainty in Rare Neurodegenerative Diseases: The Example of Autosomal-Recessive Spastic Ataxia Charlevoix Saguenay (ARSACS)","authors":"Niels Hendrickx, France Mentré, Andreas Traschütz, Cynthia Gagnon, Rebecca Schüle, Matthis Synofzik, Emmanuelle Comets","doi":"10.1208/s12248-024-00925-7","DOIUrl":null,"url":null,"abstract":"<p>The aim of this study was to develop a model to predict individual subject disease trajectories including parameter uncertainty and accounting for missing data in rare neurological diseases, showcased by the ultra-rare disease Autosomal-Recessive Spastic Ataxia Charlevoix Saguenay (ARSACS). We modelled the change in SARA (Scale for Assessment and Rating of Ataxia) score <i>versus</i> Time Since Onset of symptoms using non-linear mixed effect models for a population of 173 patients with ARSACS included in the prospective real-world multicenter Autosomal Recessive Cerebellar Ataxia (ARCA) registry. We used the Multivariate Imputation Chained Equation (MICE) algorithm to impute missing covariates, and a covariate selection procedure with a pooled p-value to account for the multiply imputed data sets. We then investigated the impact of covariates and population parameter uncertainty on the prediction of the individual trajectories up to 5 years after their last visit. A four-parameter logistic function was selected. Men were estimated to have a 25% lower SARA score at disease onset and a moderately higher maximum SARA score, and time to progression (T50) was estimated to be 35% lower in patients with age of onset over 15 years. The population disease progression rate started slowly at 0.1 points per year peaking to a maximum of 0.8 points per year (at 36.8 years since onset of symptoms). The prediction intervals for SARA scores 5 years after the last visit were large (median 7.4 points, Q1-Q3: 6.4–8.5); their size was mostly driven by individual parameter uncertainty and individual disease progression rate at that time.</p><h3 data-test=\"abstract-sub-heading\">Graphical Abstract</h3>\n","PeriodicalId":501692,"journal":{"name":"The AAPS Journal","volume":"49 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The AAPS Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1208/s12248-024-00925-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
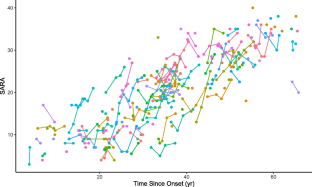
The aim of this study was to develop a model to predict individual subject disease trajectories including parameter uncertainty and accounting for missing data in rare neurological diseases, showcased by the ultra-rare disease Autosomal-Recessive Spastic Ataxia Charlevoix Saguenay (ARSACS). We modelled the change in SARA (Scale for Assessment and Rating of Ataxia) score versus Time Since Onset of symptoms using non-linear mixed effect models for a population of 173 patients with ARSACS included in the prospective real-world multicenter Autosomal Recessive Cerebellar Ataxia (ARCA) registry. We used the Multivariate Imputation Chained Equation (MICE) algorithm to impute missing covariates, and a covariate selection procedure with a pooled p-value to account for the multiply imputed data sets. We then investigated the impact of covariates and population parameter uncertainty on the prediction of the individual trajectories up to 5 years after their last visit. A four-parameter logistic function was selected. Men were estimated to have a 25% lower SARA score at disease onset and a moderately higher maximum SARA score, and time to progression (T50) was estimated to be 35% lower in patients with age of onset over 15 years. The population disease progression rate started slowly at 0.1 points per year peaking to a maximum of 0.8 points per year (at 36.8 years since onset of symptoms). The prediction intervals for SARA scores 5 years after the last visit were large (median 7.4 points, Q1-Q3: 6.4–8.5); their size was mostly driven by individual parameter uncertainty and individual disease progression rate at that time.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
