Kristen M. Quinn, Louis T. Runge, Claire Griffiths, Hannah Harris, Heidi Pieper, Michael Meara, Ben Poulose, Vimal Narula, David Renton, Courtney Collins, Alan Harzman, Syed Husain
{"title":"Laparoscopic vs robotic inguinal hernia repair: a comparison of learning curves and skill transference in general surgery residents","authors":"Kristen M. Quinn, Louis T. Runge, Claire Griffiths, Hannah Harris, Heidi Pieper, Michael Meara, Ben Poulose, Vimal Narula, David Renton, Courtney Collins, Alan Harzman, Syed Husain","doi":"10.1007/s00464-024-10860-5","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Background</h3><p>There is no consensus on whether laparoscopic experience should be a prerequisite for robotic training. Further, there is limited information on skill transference between laparoscopic and robotic techniques. This study focused on the general surgery residents’ learning curve and skill transference within the two minimally invasive platforms.</p><h3 data-test=\"abstract-sub-heading\">Methods</h3><p>General surgery residents were observed during the performance of laparoscopic and robotic inguinal hernia repairs. The recorded data included objective measures (operative time, resident participation indicated by percent active time on console or laparoscopy relative to total case time, number of handoffs between the resident and attending), and subjective evaluations (preceptor and trainee assessments of operative performance) while controlling for case complexity, patient comorbidities, and residents’ prior operative experience. Wilcoxon two-sample tests and Pearson Correlation coefficients were used for analysis.</p><h3 data-test=\"abstract-sub-heading\">Results</h3><p>Twenty laparoscopic and forty-four robotic cases were observed. Mean operative times were 90 min for robotic and 95 min for laparoscopic cases (<i>P</i> = 0.4590). Residents’ active participation time was 66% on the robotic platform and 37% for laparoscopic (<i>P</i> = < 0.0001). On average, hand-offs occurred 9.7 times during robotic cases and 6.3 times during laparoscopic cases (<i>P</i> = 0.0131). The mean number of cases per resident was 5.86 robotic and 1.67 laparoscopic (<i>P</i> = 0.0312). For robotic cases, there was a strong correlation between percent active resident participation and their prior robotic experience (<i>r</i> = 0.78) while there was a weaker correlation with prior laparoscopic experience (<i>r</i> = 0.47). On the other hand, prior robotic experience had minimal correlation with the percent active resident participation in laparoscopic cases (<i>r</i> = 0.12) and a weak correlation with prior laparoscopic experience (<i>r</i> = 0.37).</p><h3 data-test=\"abstract-sub-heading\">Conclusion</h3><p>The robotic platform may be a more effective teaching tool with a higher degree of entrustability indicated by the higher mean resident participation. We observed a greater degree of skill transference from laparoscopy to the robot, indicated by a higher degree of correlation between the resident’s prior laparoscopic experience and the percent console time in robotic cases. There was minimal correlation between residents’ prior robotic experience and their participation in laparoscopic cases. Our findings suggest that the learning curve for the robot may be shorter as prior robotic experience had a much stronger association with future robotic performance compared to the association observed in laparoscopy.</p>","PeriodicalId":501625,"journal":{"name":"Surgical Endoscopy","volume":"25 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Endoscopy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s00464-024-10860-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
There is no consensus on whether laparoscopic experience should be a prerequisite for robotic training. Further, there is limited information on skill transference between laparoscopic and robotic techniques. This study focused on the general surgery residents’ learning curve and skill transference within the two minimally invasive platforms.
Methods
General surgery residents were observed during the performance of laparoscopic and robotic inguinal hernia repairs. The recorded data included objective measures (operative time, resident participation indicated by percent active time on console or laparoscopy relative to total case time, number of handoffs between the resident and attending), and subjective evaluations (preceptor and trainee assessments of operative performance) while controlling for case complexity, patient comorbidities, and residents’ prior operative experience. Wilcoxon two-sample tests and Pearson Correlation coefficients were used for analysis.
Results
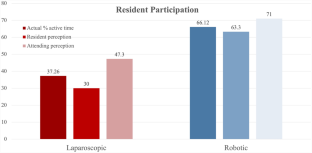
Twenty laparoscopic and forty-four robotic cases were observed. Mean operative times were 90 min for robotic and 95 min for laparoscopic cases (P = 0.4590). Residents’ active participation time was 66% on the robotic platform and 37% for laparoscopic (P = < 0.0001). On average, hand-offs occurred 9.7 times during robotic cases and 6.3 times during laparoscopic cases (P = 0.0131). The mean number of cases per resident was 5.86 robotic and 1.67 laparoscopic (P = 0.0312). For robotic cases, there was a strong correlation between percent active resident participation and their prior robotic experience (r = 0.78) while there was a weaker correlation with prior laparoscopic experience (r = 0.47). On the other hand, prior robotic experience had minimal correlation with the percent active resident participation in laparoscopic cases (r = 0.12) and a weak correlation with prior laparoscopic experience (r = 0.37).
Conclusion
The robotic platform may be a more effective teaching tool with a higher degree of entrustability indicated by the higher mean resident participation. We observed a greater degree of skill transference from laparoscopy to the robot, indicated by a higher degree of correlation between the resident’s prior laparoscopic experience and the percent console time in robotic cases. There was minimal correlation between residents’ prior robotic experience and their participation in laparoscopic cases. Our findings suggest that the learning curve for the robot may be shorter as prior robotic experience had a much stronger association with future robotic performance compared to the association observed in laparoscopy.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
