Sam Maleki BPharm, MPharm Prac, Galahad Gu BPharm (Hons), MPharm Prac, Paul Buntine MBBS (Hons), MClinRes, FACEM, Mazdak Zamani PharmD, MHM, Cert IV TAE, CHM, Violet Zhu BPharm (Hons), Grad Cert Pharm Prac, Kayin Chan BPharm, Catherine Martin BSc (Hons), MBiostats, PhD, Anne Goulopoulos BPharm (Hons), Grad Cert Pharm Prac, MClin Pharm, Adv Prac Pharm
{"title":"The effect of an extended-hours ED clinical pharmacy service on admission medication prescribing errors","authors":"Sam Maleki BPharm, MPharm Prac, Galahad Gu BPharm (Hons), MPharm Prac, Paul Buntine MBBS (Hons), MClinRes, FACEM, Mazdak Zamani PharmD, MHM, Cert IV TAE, CHM, Violet Zhu BPharm (Hons), Grad Cert Pharm Prac, Kayin Chan BPharm, Catherine Martin BSc (Hons), MBiostats, PhD, Anne Goulopoulos BPharm (Hons), Grad Cert Pharm Prac, MClin Pharm, Adv Prac Pharm","doi":"10.1111/1742-6723.14415","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>The aim of this study was to determine the effect of a 7-day extended-hours clinical pharmacy service in the ED on medication prescribing errors upon hospital admission and time to medication reconciliation.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>In this retrospective observational study, high-needs patients reviewed by ED pharmacists were compared against those not reviewed, to determine if the service was associated with reduction in admission medication errors. The primary outcome was the rate of medication errors. Errors were independently rated by two senior clinicians using a risk-probability matrix. Secondary outcomes included service's impact on time to best possible medication history (BPMH) and medication reconciliation.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>There were 242 patients who met the inclusion criteria: 105 intervention <i>vs</i> 137 control. In the intervention arm, 74 patients had at least 1 medication error compared with 113 in the control arm (total errors 206 <i>vs</i> 407). The error rate per 10 medications (interquartile range) was 1.4 (0, 2.9) in the intervention arm compared with 2.7 (1.2, 4.3) in the control arm (risk ratio 0.66 [95% confidence interval: 0.56–0.78]; <i>P</i> < 0.001). There were 33 moderate-risk and no high-risk errors (intervention), compared with 84 moderate-risk and 3 high-risk errors (control). Percent agreement was 98.98% (weighted kappa: 0.62). Time to BPMH and medication reconciliation were reduced from 40.5 and 45.0 h to 7.8 and 40.0 h, respectively.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The 7-day extended-hours ED clinical pharmacy service was associated with a reduction in medication prescribing errors in high-needs patients and improved time to BPMH and medication reconciliation.</p>\n </section>\n </div>","PeriodicalId":11604,"journal":{"name":"Emergency Medicine Australasia","volume":"36 5","pages":"688-694"},"PeriodicalIF":1.4000,"publicationDate":"2024-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emergency Medicine Australasia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1742-6723.14415","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
The aim of this study was to determine the effect of a 7-day extended-hours clinical pharmacy service in the ED on medication prescribing errors upon hospital admission and time to medication reconciliation.
Methods
In this retrospective observational study, high-needs patients reviewed by ED pharmacists were compared against those not reviewed, to determine if the service was associated with reduction in admission medication errors. The primary outcome was the rate of medication errors. Errors were independently rated by two senior clinicians using a risk-probability matrix. Secondary outcomes included service's impact on time to best possible medication history (BPMH) and medication reconciliation.
Results
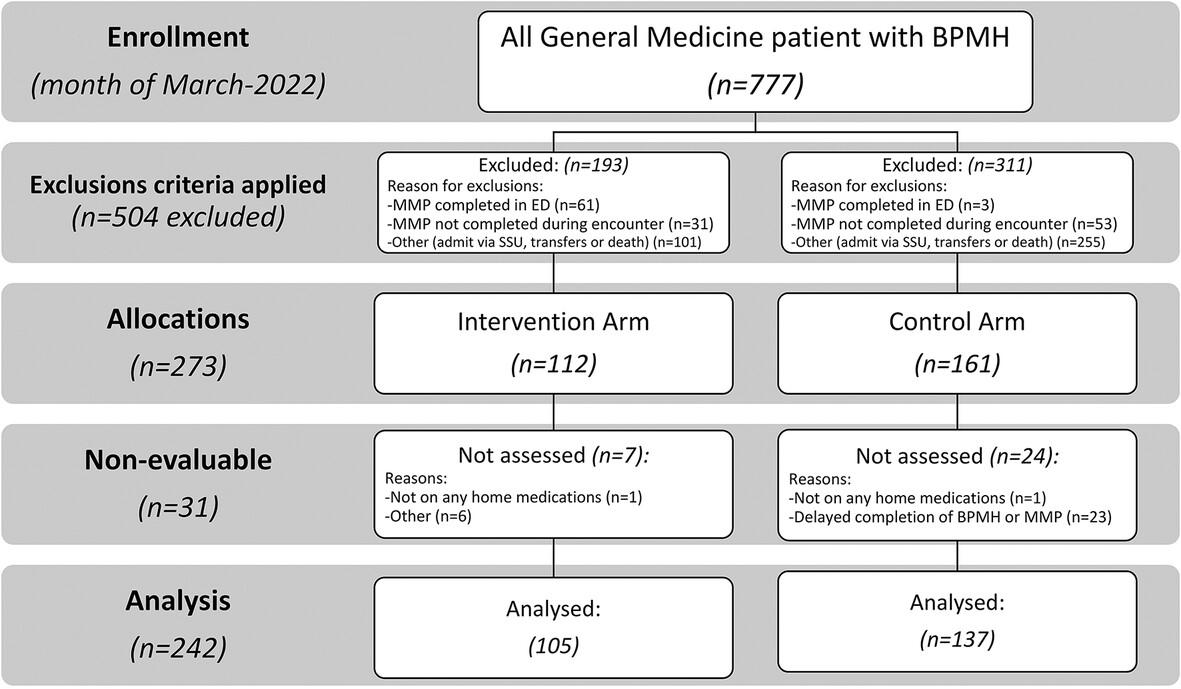
There were 242 patients who met the inclusion criteria: 105 intervention vs 137 control. In the intervention arm, 74 patients had at least 1 medication error compared with 113 in the control arm (total errors 206 vs 407). The error rate per 10 medications (interquartile range) was 1.4 (0, 2.9) in the intervention arm compared with 2.7 (1.2, 4.3) in the control arm (risk ratio 0.66 [95% confidence interval: 0.56–0.78]; P < 0.001). There were 33 moderate-risk and no high-risk errors (intervention), compared with 84 moderate-risk and 3 high-risk errors (control). Percent agreement was 98.98% (weighted kappa: 0.62). Time to BPMH and medication reconciliation were reduced from 40.5 and 45.0 h to 7.8 and 40.0 h, respectively.
Conclusions
The 7-day extended-hours ED clinical pharmacy service was associated with a reduction in medication prescribing errors in high-needs patients and improved time to BPMH and medication reconciliation.
期刊介绍:
Emergency Medicine Australasia is the official journal of the Australasian College for Emergency Medicine (ACEM) and the Australasian Society for Emergency Medicine (ASEM), and publishes original articles dealing with all aspects of clinical practice, research, education and experiences in emergency medicine.
Original articles are published under the following sections: Original Research, Paediatric Emergency Medicine, Disaster Medicine, Education and Training, Ethics, International Emergency Medicine, Management and Quality, Medicolegal Matters, Prehospital Care, Public Health, Rural and Remote Care, Technology, Toxicology and Trauma. Accepted papers become the copyright of the journal.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
