{"title":"Diabetes mellitus with severe insulin resistance in a young male patient with a heterozygous pathogenic <i>IRS1</i> frameshift variant.","authors":"Yamato Osawa, Nobutaka Ichiwata, Junko Kenmotsu, Tsuyoshi Okada, Yohei Masunaga, Tsutomu Ogata, Ichiro Morioka, Tatsuhiko Urakami","doi":"10.1297/cpe.2023-0081","DOIUrl":null,"url":null,"abstract":"<p><p>We present the case of a young male patient (height, 158.1 cm [+3.3 standard deviation (SD)]; weight, 63.7 kg [body mass index, 25.5]) with diabetes mellitus and severe insulin resistance associated with a heterozygous pathogenic insulin receptor substrate 1 (<i>IRS1</i>) frameshift mutation. The patient also had severe acanthosis nigricans. Notably, the patient's father was undergoing treatment with high doses of insulin for diabetes mellitus, and had been experiencing angina pectoris. Laboratory data showed a fasting plasma glucose level of 88 mg/dL, hemoglobin A1C (HbA1c) of 7.4%, fasting insulin level of 43.1 µg/mL, and a homeostasis model assessment-insulin resistance (HOMA-IR) score of 9.36, indicating hyperinsulinism. Oral glucose tolerance test revealed a diabetic pattern and insulin hypersecretion. In addition, the patient had hyperlipidemia. Genetic studies revealed a heterozygous frameshift variant of <i>IRS1</i> [NM_005544.3:c.1791dupG:p.(His598Alafs*13)] in the patient and his father, which can impair the binding and activation of phosphoinositide 3 (PI-3) kinase and defectively mediate the translocation of glucose transporter type 4 (GLUT4) in adipose tissues, possibly leading to glucose intolerance. Therefore, this variant may be disease causing. After confirming <i>IRS1</i> mutation, metformin was administered, and physical exercise and dietary management were initiated; metformin was well tolerated, and optimal glycemic control was maintained.</p>","PeriodicalId":10678,"journal":{"name":"Clinical Pediatric Endocrinology","volume":"33 2","pages":"87-93"},"PeriodicalIF":1.2000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10985017/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Pediatric Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1297/cpe.2023-0081","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/23 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
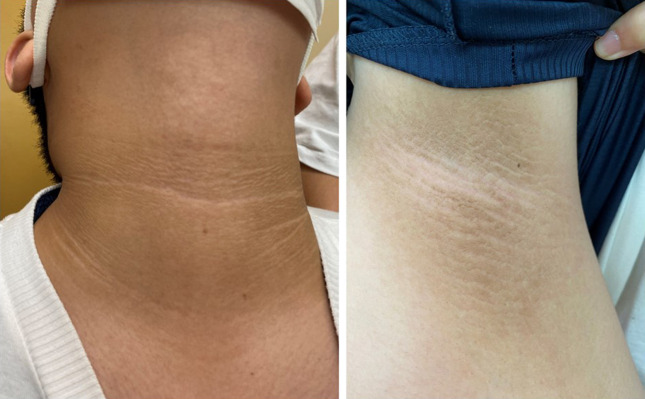
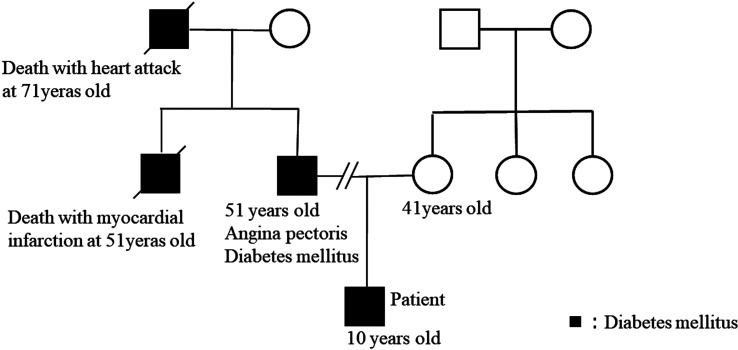
We present the case of a young male patient (height, 158.1 cm [+3.3 standard deviation (SD)]; weight, 63.7 kg [body mass index, 25.5]) with diabetes mellitus and severe insulin resistance associated with a heterozygous pathogenic insulin receptor substrate 1 (IRS1) frameshift mutation. The patient also had severe acanthosis nigricans. Notably, the patient's father was undergoing treatment with high doses of insulin for diabetes mellitus, and had been experiencing angina pectoris. Laboratory data showed a fasting plasma glucose level of 88 mg/dL, hemoglobin A1C (HbA1c) of 7.4%, fasting insulin level of 43.1 µg/mL, and a homeostasis model assessment-insulin resistance (HOMA-IR) score of 9.36, indicating hyperinsulinism. Oral glucose tolerance test revealed a diabetic pattern and insulin hypersecretion. In addition, the patient had hyperlipidemia. Genetic studies revealed a heterozygous frameshift variant of IRS1 [NM_005544.3:c.1791dupG:p.(His598Alafs*13)] in the patient and his father, which can impair the binding and activation of phosphoinositide 3 (PI-3) kinase and defectively mediate the translocation of glucose transporter type 4 (GLUT4) in adipose tissues, possibly leading to glucose intolerance. Therefore, this variant may be disease causing. After confirming IRS1 mutation, metformin was administered, and physical exercise and dietary management were initiated; metformin was well tolerated, and optimal glycemic control was maintained.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
