Gerald Musa, Medetbek Dzhumabekovich Abakirov, Gennady E Chmutin, Samat Temirbekovich Mamyrbaev, Manuel De Jesus Encarnacion Ramirez, Kachinga Sichizya, Alexander V Kim, Gennady I Antonov, Egor G Chmutin, Dmitri V Hovrin, Mihail V Slabov, Bipin Chaurasia
{"title":"Advancing insights into recurrent lumbar disc herniation: A comparative analysis of surgical approaches and a new classification.","authors":"Gerald Musa, Medetbek Dzhumabekovich Abakirov, Gennady E Chmutin, Samat Temirbekovich Mamyrbaev, Manuel De Jesus Encarnacion Ramirez, Kachinga Sichizya, Alexander V Kim, Gennady I Antonov, Egor G Chmutin, Dmitri V Hovrin, Mihail V Slabov, Bipin Chaurasia","doi":"10.4103/jcvjs.jcvjs_177_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The management of recurrent lumbar disc herniation (rLDH) lacks a consensus. Consequently, the choice between repeat microdiscectomy (MD) without fusion, discectomy with fusion, or endoscopic discectomy without fusion typically hinges on the surgeon's expertise. This study conducts a comparative analysis of postoperative outcomes among these three techniques and proposes a straightforward classification system for rLDH aimed at optimizing management.</p><p><strong>Patients and methods: </strong>We examined the patients treated for rLDH at our institution. Based on the presence of facet resection, Modic-2 changes, and segmental instability, they patients were categorized into three groups: Types I, II, and III rLDH managed by repeat MD without fusion, MD with transforaminal lumbar interbody fusion (TLIF) (MD + TLIF), and transforaminal endoscopic discectomy (TFED), respectively.</p><p><strong>Results: </strong>A total of 127 patients were included: 52 underwent MD + TLIF, 50 underwent MD alone, and 25 underwent TFED. Recurrence rates were 20%, 12%, and 0% for MD alone, TFED, and MD + TLIF, respectively. A facetectomy exceeding 75% correlated with an 84.6% recurrence risk, while segmental instability correlated with a 100% recurrence rate. Modic-2 changes were identified in 86.7% and 100% of patients experiencing recurrence following MD and TFED, respectively. TFED exhibited the lowest risk of durotomy (4%), the shortest operative time (70.80 ± 16.5), the least blood loss (33.60 ± 8.1), and the most favorable Visual Analog Scale score, and Oswestry Disability Index quality of life assessment at 2 years. No statistically significant differences were observed in these parameters between MD alone and MD + TLIF. Based on this analysis, a novel classification system for recurrent disc herniation was proposed.</p><p><strong>Conclusion: </strong>In young patients without segmental instability, prior facetectomy, and Modic-2 changes, TFED was available should take precedence over repeat MD alone. However, for patients with segmental instability, MD + TLIF is recommended. The suggested classification system has the potential to enhance patient selection and overall outcomes.</p>","PeriodicalId":51721,"journal":{"name":"Journal of Craniovertebral Junction and Spine","volume":"15 1","pages":"66-73"},"PeriodicalIF":1.3000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11029108/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Craniovertebral Junction and Spine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcvjs.jcvjs_177_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The management of recurrent lumbar disc herniation (rLDH) lacks a consensus. Consequently, the choice between repeat microdiscectomy (MD) without fusion, discectomy with fusion, or endoscopic discectomy without fusion typically hinges on the surgeon's expertise. This study conducts a comparative analysis of postoperative outcomes among these three techniques and proposes a straightforward classification system for rLDH aimed at optimizing management.
Patients and methods: We examined the patients treated for rLDH at our institution. Based on the presence of facet resection, Modic-2 changes, and segmental instability, they patients were categorized into three groups: Types I, II, and III rLDH managed by repeat MD without fusion, MD with transforaminal lumbar interbody fusion (TLIF) (MD + TLIF), and transforaminal endoscopic discectomy (TFED), respectively.
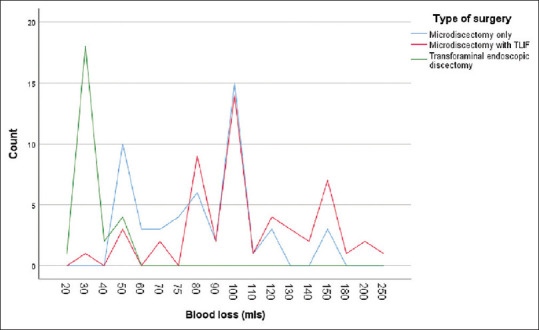
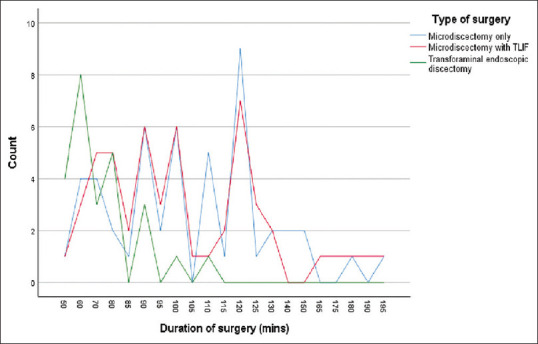
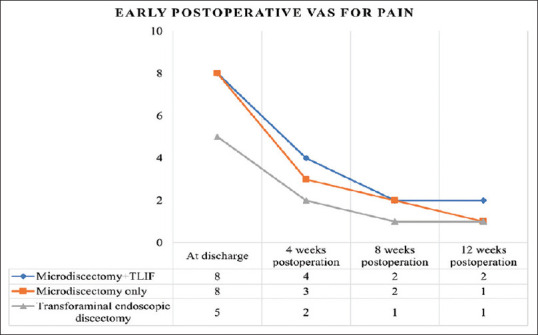
Results: A total of 127 patients were included: 52 underwent MD + TLIF, 50 underwent MD alone, and 25 underwent TFED. Recurrence rates were 20%, 12%, and 0% for MD alone, TFED, and MD + TLIF, respectively. A facetectomy exceeding 75% correlated with an 84.6% recurrence risk, while segmental instability correlated with a 100% recurrence rate. Modic-2 changes were identified in 86.7% and 100% of patients experiencing recurrence following MD and TFED, respectively. TFED exhibited the lowest risk of durotomy (4%), the shortest operative time (70.80 ± 16.5), the least blood loss (33.60 ± 8.1), and the most favorable Visual Analog Scale score, and Oswestry Disability Index quality of life assessment at 2 years. No statistically significant differences were observed in these parameters between MD alone and MD + TLIF. Based on this analysis, a novel classification system for recurrent disc herniation was proposed.
Conclusion: In young patients without segmental instability, prior facetectomy, and Modic-2 changes, TFED was available should take precedence over repeat MD alone. However, for patients with segmental instability, MD + TLIF is recommended. The suggested classification system has the potential to enhance patient selection and overall outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
