Giulia Stronati, Federico Guerra, Devis Benfaremo, Cristina Dichiara, Federico Paolini, Gianmarco Bastianoni, Leonardo Brugiatelli, Michele Alfieri, Paolo Compagnucci, Antonio Dello Russo, Gianluca Moroncini
{"title":"Speckle-tracking global longitudinal strain predicts death and cardiovascular events in patients with systemic sclerosis.","authors":"Giulia Stronati, Federico Guerra, Devis Benfaremo, Cristina Dichiara, Federico Paolini, Gianmarco Bastianoni, Leonardo Brugiatelli, Michele Alfieri, Paolo Compagnucci, Antonio Dello Russo, Gianluca Moroncini","doi":"10.1093/ehjopen/oeae023","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Albeit often asymptomatic, heart involvement in systemic sclerosis (SSc) represents a negative prognostic factor, accounting for nearly one-fourth of all deaths. Global longitudinal strain (GLS) is accurate in detecting heart involvement in patients with SSc and no overt cardiac disease and allows early detection and longitudinal monitoring, but its association with clinical endpoints has not been tested so far. The primary outcome was the association between left and right GLS and mortality for all causes. The secondary outcome was the association between left and right GLS and hospitalizations.</p><p><strong>Methods and results: </strong>A prospective longitudinal study enrolling all consecutive patients with SSc without structural heart disease or previous cardiovascular event.A total of 164 patients were enrolled, of whom 19 (11.5%) died during follow-up and 48 (29.3%) were hospitalized. Both left (LV) and right ventricle (RV) GLS at enrolment were independently associated with an increased risk of death for all causes and hospitalizations. Patients with biventricular GLS impairment, respectively, had a 4.2-, 4.9-, and 13.9-fold increased risk of death when compared with patients with only LV, only RV, or no impairment (<i>P</i> < 0.001). The incidence of hospitalization in patients with biventricular GLS impairment was nearly four times higher when compared with patients with only LV or only RV impairment, and nine times higher when compared with normal biventricular GLS (<i>P</i> < 0.001).</p><p><strong>Conclusion: </strong>Biventricular GLS is associated with an increased risk of death and hospitalization in patients with SSc during a median of 3-year follow-up, acting as a reliable and accurate prognostic tool in everyday practice.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"4 2","pages":"oeae023"},"PeriodicalIF":0.0000,"publicationDate":"2024-04-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11032194/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
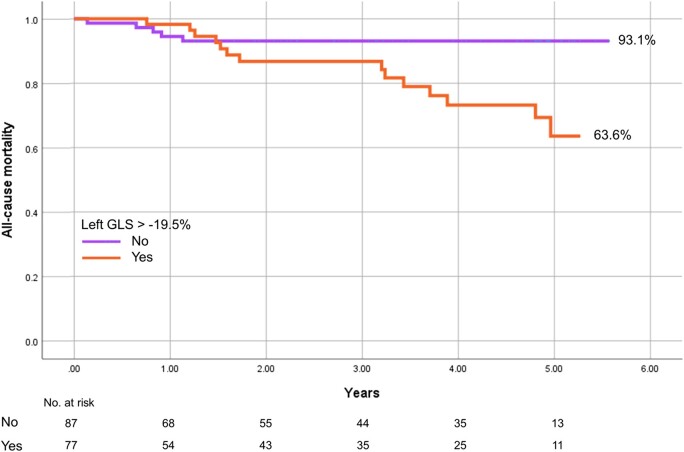
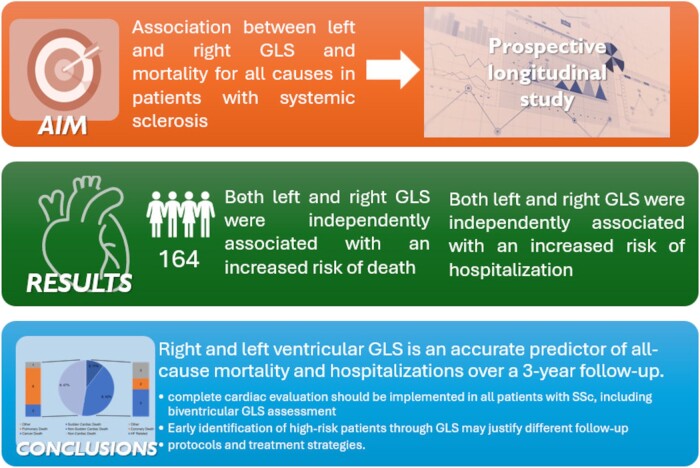
Aims: Albeit often asymptomatic, heart involvement in systemic sclerosis (SSc) represents a negative prognostic factor, accounting for nearly one-fourth of all deaths. Global longitudinal strain (GLS) is accurate in detecting heart involvement in patients with SSc and no overt cardiac disease and allows early detection and longitudinal monitoring, but its association with clinical endpoints has not been tested so far. The primary outcome was the association between left and right GLS and mortality for all causes. The secondary outcome was the association between left and right GLS and hospitalizations.
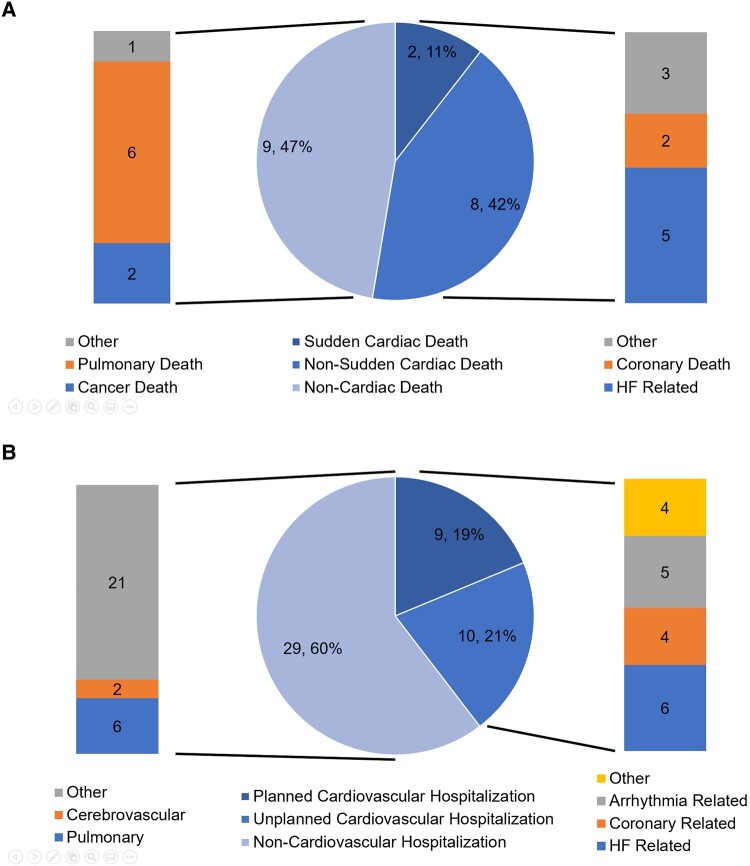
Methods and results: A prospective longitudinal study enrolling all consecutive patients with SSc without structural heart disease or previous cardiovascular event.A total of 164 patients were enrolled, of whom 19 (11.5%) died during follow-up and 48 (29.3%) were hospitalized. Both left (LV) and right ventricle (RV) GLS at enrolment were independently associated with an increased risk of death for all causes and hospitalizations. Patients with biventricular GLS impairment, respectively, had a 4.2-, 4.9-, and 13.9-fold increased risk of death when compared with patients with only LV, only RV, or no impairment (P < 0.001). The incidence of hospitalization in patients with biventricular GLS impairment was nearly four times higher when compared with patients with only LV or only RV impairment, and nine times higher when compared with normal biventricular GLS (P < 0.001).
Conclusion: Biventricular GLS is associated with an increased risk of death and hospitalization in patients with SSc during a median of 3-year follow-up, acting as a reliable and accurate prognostic tool in everyday practice.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
