Effective treatment of MET exon 14 skipping mutation-positive non-small cell lung cancer using capmatinib following serious maculopapular rash caused by two MET inhibitors: a case report.
{"title":"Effective treatment of <i>MET</i> exon 14 skipping mutation-positive non-small cell lung cancer using capmatinib following serious maculopapular rash caused by two MET inhibitors: a case report.","authors":"Fumihiro Kashizaki, Shunsuke Okazaki, Nanami Tsuchiya, Hao Chen, Harumi Koizumi, Kenichi Takahashi","doi":"10.21037/acr-23-181","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Multi-gene panel testing and advancements in molecular targeted therapy have improved the overall survival of patients with driver mutation-positive non-small cell lung cancer (NSCLC). Mesenchymal-epithelial transition factor (<i>MET</i>) exon 14 skipping mutation-positive NSCLC, which remains untreated with MET inhibitors, shows a poorer prognosis than do cases of NSCLC without <i>MET</i> mutations. However, serious treatment-related adverse events (TRAEs) act as substantial treatment barriers.</p><p><strong>Case description: </strong>Herein, we report a case of advanced NSCLC in a male in his 40s with <i>MET</i> exon 14 skipping mutation. A MET-inhibitory investigational drug was administered as first-line treatment; the development of grade 3 maculopapular rash necessitated dose reduction, which resulted in disease progression. Tepotinib was then administered with dexamethasone as a third-line treatment but was discontinued owing to the re-development of the grade 3 maculopapular rash. Finally, capmatinib administration as the fifth-line treatment appeared partially effective, with no serious adverse events. The patient could successfully resume work.</p><p><strong>Conclusions: </strong>This is the first report of <i>MET</i> exon 14 skipping mutation-positive NSCLC wherein partial response was achieved without severe TRAEs by alternating between two MET inhibitors. If no alternative treatments are available, cautious repeated re-administration of MET inhibitors after resolving serious rashes can be considered a potential approach.</p>","PeriodicalId":29752,"journal":{"name":"AME Case Reports","volume":"8 ","pages":"42"},"PeriodicalIF":0.6000,"publicationDate":"2024-03-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11071010/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AME Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/acr-23-181","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Multi-gene panel testing and advancements in molecular targeted therapy have improved the overall survival of patients with driver mutation-positive non-small cell lung cancer (NSCLC). Mesenchymal-epithelial transition factor (MET) exon 14 skipping mutation-positive NSCLC, which remains untreated with MET inhibitors, shows a poorer prognosis than do cases of NSCLC without MET mutations. However, serious treatment-related adverse events (TRAEs) act as substantial treatment barriers.
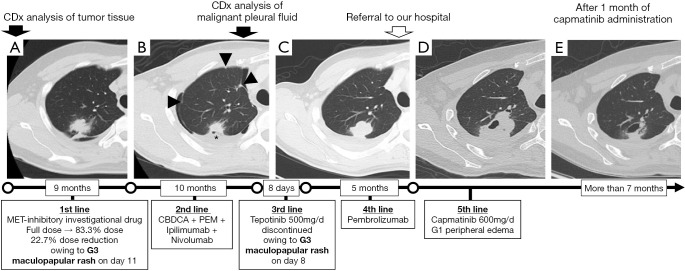
Case description: Herein, we report a case of advanced NSCLC in a male in his 40s with MET exon 14 skipping mutation. A MET-inhibitory investigational drug was administered as first-line treatment; the development of grade 3 maculopapular rash necessitated dose reduction, which resulted in disease progression. Tepotinib was then administered with dexamethasone as a third-line treatment but was discontinued owing to the re-development of the grade 3 maculopapular rash. Finally, capmatinib administration as the fifth-line treatment appeared partially effective, with no serious adverse events. The patient could successfully resume work.
Conclusions: This is the first report of MET exon 14 skipping mutation-positive NSCLC wherein partial response was achieved without severe TRAEs by alternating between two MET inhibitors. If no alternative treatments are available, cautious repeated re-administration of MET inhibitors after resolving serious rashes can be considered a potential approach.
背景:多基因面板检测和分子靶向治疗的进步提高了驱动基因突变阳性非小细胞肺癌(NSCLC)患者的总生存率。间充质-上皮转化因子(MET)第14外显子跳越突变阳性的非小细胞肺癌患者仍未接受MET抑制剂治疗,与无MET突变的非小细胞肺癌患者相比,其预后较差。然而,严重的治疗相关不良事件(TRAEs)成为治疗的实质性障碍:在此,我们报告了一例 40 多岁男性晚期 NSCLC 病例,患者存在 MET 第 14 号外显子跳越突变。在一线治疗中使用了一种 MET 抑制性试验药物;由于出现了 3 级斑丘疹,不得不减少剂量,结果导致疾病进展。随后,特博替尼与地塞米松一起作为三线治疗药物,但由于再次出现3级斑丘疹而停药。最后,卡帕替尼作为五线治疗似乎部分有效,没有出现严重不良反应。患者可以顺利恢复工作:这是首例通过交替使用两种 MET 抑制剂获得部分应答且无严重 TRAEs 的 MET 14 外显子跳过突变阳性 NSCLC 报告。如果没有其他治疗方法,在解决严重皮疹问题后谨慎地反复使用 MET 抑制剂不失为一种可行的方法。



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
