Ashna I E Ramautar, Ana Navas, Elizabeth M Winter, Herman M Kroon, Frits Smit, Dennis Vriens, Neveen A T Hamdy, Natasha M Appelman-Dijkstra
{"title":"Defining the imaging diagnostic criteria for adult chronic non-bacterial osteitis.","authors":"Ashna I E Ramautar, Ana Navas, Elizabeth M Winter, Herman M Kroon, Frits Smit, Dennis Vriens, Neveen A T Hamdy, Natasha M Appelman-Dijkstra","doi":"10.1093/jbmrpl/ziae024","DOIUrl":null,"url":null,"abstract":"<p><p>Osteitis of the sternocostoclavicular (SCC) region, referred to as sternocostoclavicular hyperostosis (SCCH), is the clinical expression of chronic non-bacterial osteitis (CNO) in adults with this rare chronic auto-inflammatory disorder of the axial skeleton. The diagnosis is based on distinctive computerized tomography (CT) features of sclerosis and hyperostosis of the SCC region, and local increases in osteoid formation visualized by high radiopharmacon uptake on skeletal scintigraphy but clear radiologic diagnostic criteria are lacking. In a cross-sectional study, CT scans and whole-body skeletal scintigraphy images obtained in 169 patients seen at the Center for Bone Quality of the Leiden University Medical Center between 2008 and 2018 with a suspected diagnosis of CNO of the SCC region were re-evaluated by 2 skeletal radiologists and 2 nuclear physicians. The diagnosis was confirmed in 118 (70%) predominantly female patients (<i>n</i> = 103, 89.2%); median age at first symptoms 45 years (range 20-73). The diagnosis was excluded in the remaining 51 \"non-CNO\" patients. Increased radiopharmacon uptake at the SCC region was observed in 82% CNO patients, with the manubrium sterni having the highest predictive ability to discriminate on both imaging modalities. The prevalence of sclerosis of the clavicles, manubrium and first ribs was significantly higher in CNO patients (<i>P</i> < 0.001). Hyperostosis was not observed in non-CNO patients. 46 CNO versus only 2 non-CNO patients had costoclavicular ligament calcification. Our findings identify CT scan features of sclerosis and hyperostosis of manubrium sterni, medial end of clavicles and first ribs, and calcification of costoclavicular ligaments, associated with increased tracer uptake on skeletal scintigraphy at the SCC region, specifically manubrium sterni, as well-defined imaging diagnostic criteria for adult CNO. Pitfalls encountered in the diagnosis of CNO are highlighted. These defined imaging diagnostic criteria for adult CNO should facilitate the diagnosis of this rare auto-inflammatory bone disease across the spectrum of its early to late stages.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"8 5","pages":"ziae024"},"PeriodicalIF":2.4000,"publicationDate":"2024-03-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11008733/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziae024","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
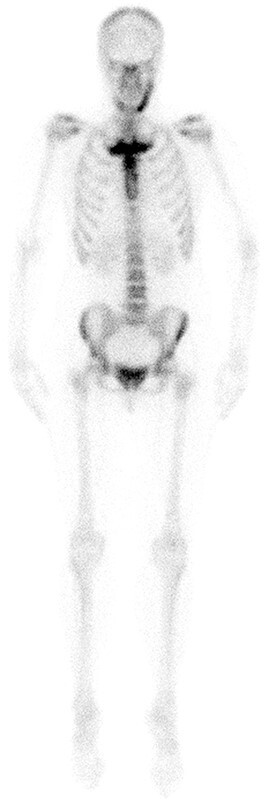
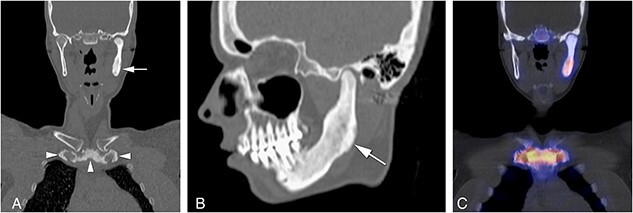
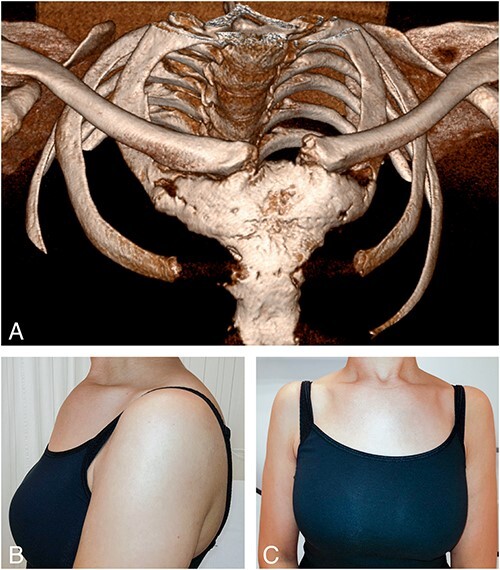
Osteitis of the sternocostoclavicular (SCC) region, referred to as sternocostoclavicular hyperostosis (SCCH), is the clinical expression of chronic non-bacterial osteitis (CNO) in adults with this rare chronic auto-inflammatory disorder of the axial skeleton. The diagnosis is based on distinctive computerized tomography (CT) features of sclerosis and hyperostosis of the SCC region, and local increases in osteoid formation visualized by high radiopharmacon uptake on skeletal scintigraphy but clear radiologic diagnostic criteria are lacking. In a cross-sectional study, CT scans and whole-body skeletal scintigraphy images obtained in 169 patients seen at the Center for Bone Quality of the Leiden University Medical Center between 2008 and 2018 with a suspected diagnosis of CNO of the SCC region were re-evaluated by 2 skeletal radiologists and 2 nuclear physicians. The diagnosis was confirmed in 118 (70%) predominantly female patients (n = 103, 89.2%); median age at first symptoms 45 years (range 20-73). The diagnosis was excluded in the remaining 51 "non-CNO" patients. Increased radiopharmacon uptake at the SCC region was observed in 82% CNO patients, with the manubrium sterni having the highest predictive ability to discriminate on both imaging modalities. The prevalence of sclerosis of the clavicles, manubrium and first ribs was significantly higher in CNO patients (P < 0.001). Hyperostosis was not observed in non-CNO patients. 46 CNO versus only 2 non-CNO patients had costoclavicular ligament calcification. Our findings identify CT scan features of sclerosis and hyperostosis of manubrium sterni, medial end of clavicles and first ribs, and calcification of costoclavicular ligaments, associated with increased tracer uptake on skeletal scintigraphy at the SCC region, specifically manubrium sterni, as well-defined imaging diagnostic criteria for adult CNO. Pitfalls encountered in the diagnosis of CNO are highlighted. These defined imaging diagnostic criteria for adult CNO should facilitate the diagnosis of this rare auto-inflammatory bone disease across the spectrum of its early to late stages.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
