{"title":"A Current Perspective on Delayed Puberty and Its Management","authors":"Ayhan Abacı, Özge Besci","doi":"10.4274/jcrpe.galenos.2024.2024-2-7","DOIUrl":null,"url":null,"abstract":"<p><p>Delayed puberty is defined as the lack of development of secondary sex characteristics in childhood. Based on a review of the literature, delayed puberty can be divided into three main categories: (i) hypergonadotropic hypogonadism (congenital and acquired); (ii) permanent hypogonadotropic hypogonadism (congenital and acquired); and (iii) transient hypogonadotropic hypogonadism [constitutional delay of growth and puberty (CDGP) and functional hypogonadotropic hypogonadism]. CDGP is the most common cause of hypogonadism in both males and females, accounting for 60% and 30% respectively. Testosterone is the primary treatment for male hypogonadism, while estrogen and progesterone are used for female hypogonadism. However, in recent years, physiological induction therapy protocols such as human chorionic gonadotropin (hCG) monotherapy, hCG + follicle-stimulating hormone combined therapy, and gonadotropin-releasing hormone infusion have been recommended for the treatment of hypogonadotropic hypogonadism to increase long-term fertility success. There is no clear consensus on treatment protocols for physiological induction treatment and its effect on fertility. This review will discuss the clinical approach to hypogonadism, as well as traditional and physiological induction protocols.</p>","PeriodicalId":48805,"journal":{"name":"Journal of Clinical Research in Pediatric Endocrinology","volume":" ","pages":"379-400"},"PeriodicalIF":1.5000,"publicationDate":"2024-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11629716/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Research in Pediatric Endocrinology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4274/jcrpe.galenos.2024.2024-2-7","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/29 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
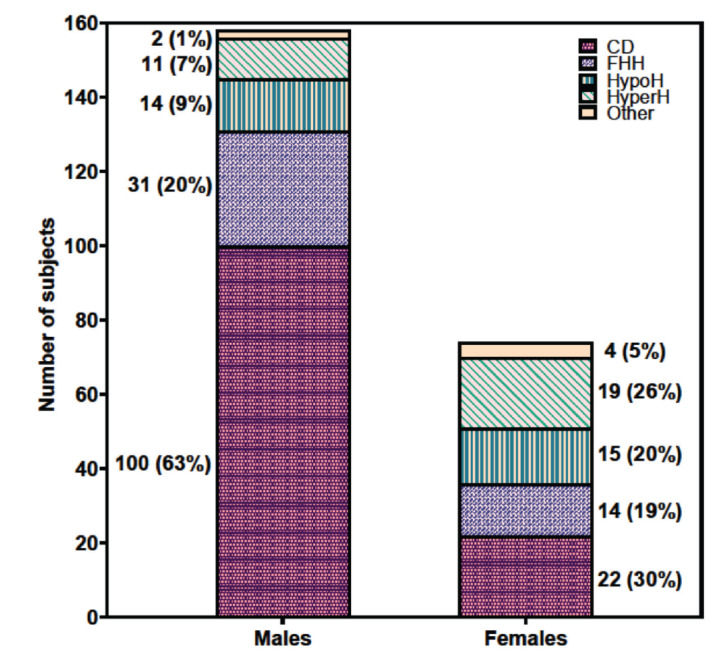
Delayed puberty is defined as the lack of development of secondary sex characteristics in childhood. Based on a review of the literature, delayed puberty can be divided into three main categories: (i) hypergonadotropic hypogonadism (congenital and acquired); (ii) permanent hypogonadotropic hypogonadism (congenital and acquired); and (iii) transient hypogonadotropic hypogonadism [constitutional delay of growth and puberty (CDGP) and functional hypogonadotropic hypogonadism]. CDGP is the most common cause of hypogonadism in both males and females, accounting for 60% and 30% respectively. Testosterone is the primary treatment for male hypogonadism, while estrogen and progesterone are used for female hypogonadism. However, in recent years, physiological induction therapy protocols such as human chorionic gonadotropin (hCG) monotherapy, hCG + follicle-stimulating hormone combined therapy, and gonadotropin-releasing hormone infusion have been recommended for the treatment of hypogonadotropic hypogonadism to increase long-term fertility success. There is no clear consensus on treatment protocols for physiological induction treatment and its effect on fertility. This review will discuss the clinical approach to hypogonadism, as well as traditional and physiological induction protocols.
期刊介绍:
The Journal of Clinical Research in Pediatric Endocrinology (JCRPE) publishes original research articles, reviews, short communications, letters, case reports and other special features related to the field of pediatric endocrinology. JCRPE is published in English by the Turkish Pediatric Endocrinology and Diabetes Society quarterly (March, June, September, December). The target audience is physicians, researchers and other healthcare professionals in all areas of pediatric endocrinology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
