Abdulraouf M Z Jijeh, Anis Fatima, Mohammad A Faraji, Hussam K Hamadah, Ghassan A Shaath
{"title":"Intracranial Pressure and Cerebral Hemodynamics in Infants Before and After Glenn Procedure.","authors":"Abdulraouf M Z Jijeh, Anis Fatima, Mohammad A Faraji, Hussam K Hamadah, Ghassan A Shaath","doi":"10.1097/CCE.0000000000001083","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This prospective cohort study aimed to investigate changes in intracranial pressure (ICP) and cerebral hemodynamics in infants with congenital heart disease undergoing the Glenn procedure, focusing on the relationship between superior vena cava pressure and estimated ICP.</p><p><strong>Design: </strong>A single-center prospective cohort study.</p><p><strong>Setting: </strong>The study was conducted in a cardiac center over 4 years (2019-2022).</p><p><strong>Patients: </strong>Twenty-seven infants with congenital heart disease scheduled for the Glenn procedure were included in the study, and detailed patient demographics and primary diagnoses were recorded.</p><p><strong>Interventions: </strong>Transcranial Doppler (TCD) ultrasound examinations were performed at three time points: baseline (preoperatively), postoperative while ventilated (within 24-48 hr), and at discharge. TCD parameters, blood pressure, and pulmonary artery pressure were measured.</p><p><strong>Measurements and main results: </strong>TCD parameters included systolic flow velocity, diastolic flow velocity (dFV), mean flow velocity (mFV), pulsatility index (PI), and resistance index. Estimated ICP and cerebral perfusion pressure (CPP) were calculated using established formulas. There was a significant postoperative increase in estimated ICP from 11 mm Hg (interquartile range [IQR], 10-16 mm Hg) to 15 mm Hg (IQR, 12-21 mm Hg) postoperatively (<i>p</i> = 0.002) with a trend toward higher CPP from 22 mm Hg (IQR, 14-30 mm Hg) to 28 mm Hg (IQR, 22-38 mm Hg) postoperatively (<i>p</i> = 0.1). TCD indices reflected alterations in cerebral hemodynamics, including decreased dFV and mFV and increased PI. Intracranial hemodynamics while on positive airway pressure and after extubation were similar.</p><p><strong>Conclusions: </strong>Glenn procedure substantially increases estimated ICP while showing a trend toward higher CPP. These findings underscore the intricate interaction between venous pressure and cerebral hemodynamics in infants undergoing the Glenn procedure. They also highlight the remarkable complexity of cerebrovascular autoregulation in maintaining stable brain perfusion under these circumstances.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"6 5","pages":"e1083"},"PeriodicalIF":2.7000,"publicationDate":"2024-04-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11057806/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001083","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: This prospective cohort study aimed to investigate changes in intracranial pressure (ICP) and cerebral hemodynamics in infants with congenital heart disease undergoing the Glenn procedure, focusing on the relationship between superior vena cava pressure and estimated ICP.
Design: A single-center prospective cohort study.
Setting: The study was conducted in a cardiac center over 4 years (2019-2022).
Patients: Twenty-seven infants with congenital heart disease scheduled for the Glenn procedure were included in the study, and detailed patient demographics and primary diagnoses were recorded.
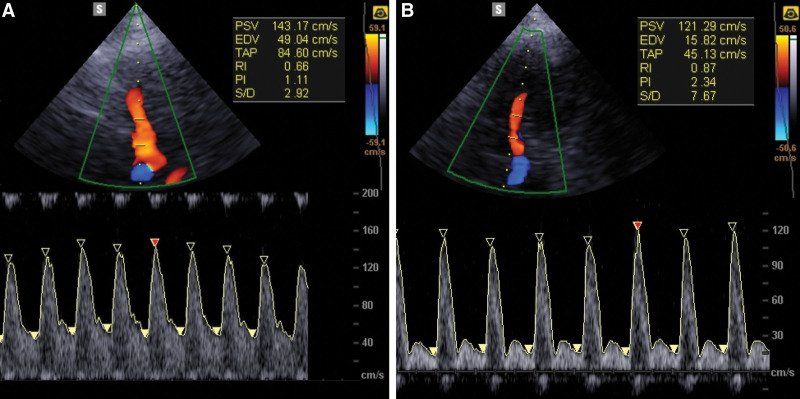
Interventions: Transcranial Doppler (TCD) ultrasound examinations were performed at three time points: baseline (preoperatively), postoperative while ventilated (within 24-48 hr), and at discharge. TCD parameters, blood pressure, and pulmonary artery pressure were measured.
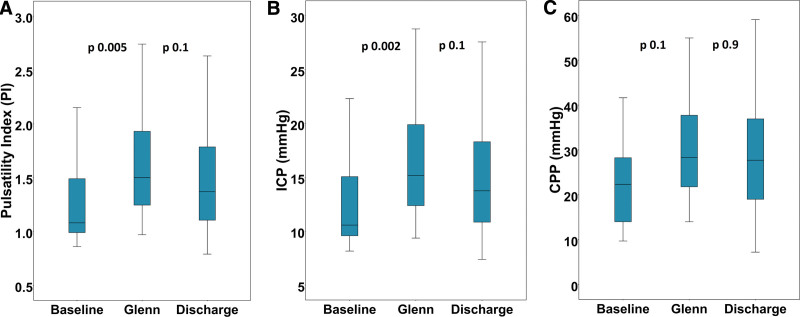
Measurements and main results: TCD parameters included systolic flow velocity, diastolic flow velocity (dFV), mean flow velocity (mFV), pulsatility index (PI), and resistance index. Estimated ICP and cerebral perfusion pressure (CPP) were calculated using established formulas. There was a significant postoperative increase in estimated ICP from 11 mm Hg (interquartile range [IQR], 10-16 mm Hg) to 15 mm Hg (IQR, 12-21 mm Hg) postoperatively (p = 0.002) with a trend toward higher CPP from 22 mm Hg (IQR, 14-30 mm Hg) to 28 mm Hg (IQR, 22-38 mm Hg) postoperatively (p = 0.1). TCD indices reflected alterations in cerebral hemodynamics, including decreased dFV and mFV and increased PI. Intracranial hemodynamics while on positive airway pressure and after extubation were similar.
Conclusions: Glenn procedure substantially increases estimated ICP while showing a trend toward higher CPP. These findings underscore the intricate interaction between venous pressure and cerebral hemodynamics in infants undergoing the Glenn procedure. They also highlight the remarkable complexity of cerebrovascular autoregulation in maintaining stable brain perfusion under these circumstances.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
