A Krelle, S Price, M M Law, S Kranz, P Shamdasani, S Kane, J Unterscheider, P Champion de Crespigny
{"title":"The Challenges of Distinguishing Different Causes of TMA in a Pregnant Kidney Transplant Recipient.","authors":"A Krelle, S Price, M M Law, S Kranz, P Shamdasani, S Kane, J Unterscheider, P Champion de Crespigny","doi":"10.1155/2024/9218637","DOIUrl":null,"url":null,"abstract":"<p><p>Thrombotic microangiopathy (TMA) reflects a syndrome of endothelial injury characterised by microangiopathic haemolytic anaemia (nonimmune), thrombocytopenia, and often end-organ dysfunction. TMA disorders are well-recognised in kidney transplant recipients, often due to an underlying genetic predisposition related to complement dysregulation, or de novo due to infection, immunosuppression toxicity, or antibody-mediated rejection. In pregnancy, TMA disorders are most commonly due to severe pre-eclampsia or HELLP, but may also be due to thrombotic thrombocytopenic purpura (TTP) or complement-mediated (atypical) haemolytic uremic syndrome (aHUS). Complement dysregulation is being recognised as playing a role in the development of preeclampsia and HELLP syndrome in addition to aHUS. Due to overlapping clinical and laboratory features, diagnosis can be difficult and delays in treatment can be life-threatening for both mother and fetus. This report describes a 32 year-old female who had two successive wanted pregnancies. The first pregnancy was terminated at 22 weeks gestation due to presumed severe preeclampsia and fetal growth restriction in the context of known chronic kidney failure due to reflux nephropathy. A living-related kidney transplant was performed to improve the chances of pregnancy resulting in a live birth. A subsequent pregnancy was complicated by progressive kidney impairment and hypertension at 22 weeks gestation. Kidney biopsy showed TMA, but the etiology was unclear. This report highlights the diagnostic dilemma of TMA in a pregnant kidney transplant recipient and a role for the anti-C5 terminal complement blockade monoclonal antibody eculizumab, in pregnancy-associated TMA, especially at a peri-viable gestation.</p>","PeriodicalId":9604,"journal":{"name":"Case Reports in Nephrology","volume":"2024 ","pages":"9218637"},"PeriodicalIF":0.0000,"publicationDate":"2024-04-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11074854/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/9218637","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
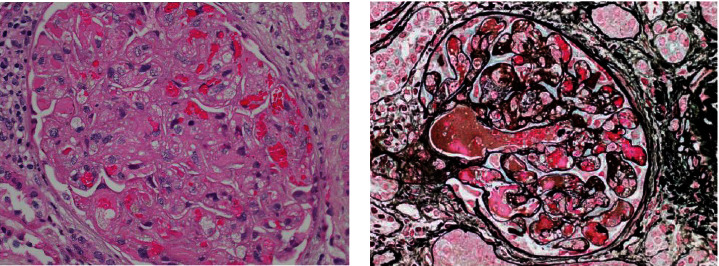
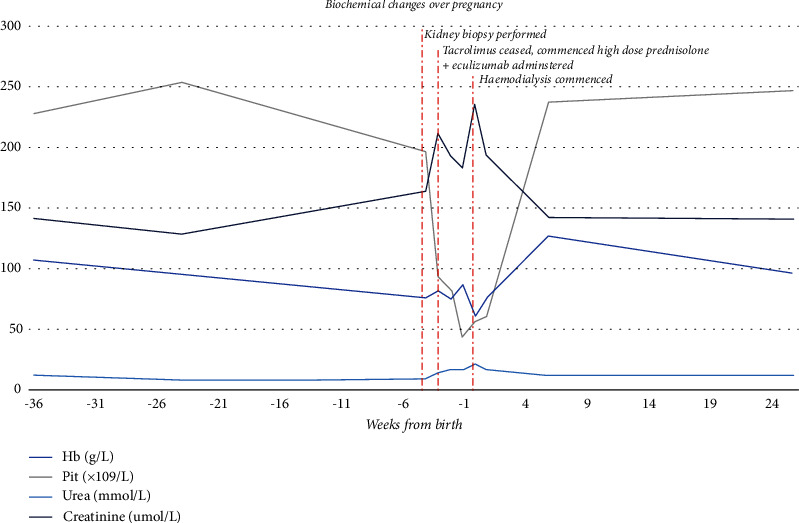
Thrombotic microangiopathy (TMA) reflects a syndrome of endothelial injury characterised by microangiopathic haemolytic anaemia (nonimmune), thrombocytopenia, and often end-organ dysfunction. TMA disorders are well-recognised in kidney transplant recipients, often due to an underlying genetic predisposition related to complement dysregulation, or de novo due to infection, immunosuppression toxicity, or antibody-mediated rejection. In pregnancy, TMA disorders are most commonly due to severe pre-eclampsia or HELLP, but may also be due to thrombotic thrombocytopenic purpura (TTP) or complement-mediated (atypical) haemolytic uremic syndrome (aHUS). Complement dysregulation is being recognised as playing a role in the development of preeclampsia and HELLP syndrome in addition to aHUS. Due to overlapping clinical and laboratory features, diagnosis can be difficult and delays in treatment can be life-threatening for both mother and fetus. This report describes a 32 year-old female who had two successive wanted pregnancies. The first pregnancy was terminated at 22 weeks gestation due to presumed severe preeclampsia and fetal growth restriction in the context of known chronic kidney failure due to reflux nephropathy. A living-related kidney transplant was performed to improve the chances of pregnancy resulting in a live birth. A subsequent pregnancy was complicated by progressive kidney impairment and hypertension at 22 weeks gestation. Kidney biopsy showed TMA, but the etiology was unclear. This report highlights the diagnostic dilemma of TMA in a pregnant kidney transplant recipient and a role for the anti-C5 terminal complement blockade monoclonal antibody eculizumab, in pregnancy-associated TMA, especially at a peri-viable gestation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
