Preoperative echocardiography as a predictor of spinal anesthesia-induced hypotension in older patients with mild left ventricular diastolic dysfunction: a retrospective observational study.
Eun Ji Park, Ah-Reum Cho, Hyae-Jin Kim, Hyeon-Jeong Lee, Soeun Jeon, Jiseok Baik, Wangseok Do, Christine Kang, Yerin Kang
{"title":"Preoperative echocardiography as a predictor of spinal anesthesia-induced hypotension in older patients with mild left ventricular diastolic dysfunction: a retrospective observational study.","authors":"Eun Ji Park, Ah-Reum Cho, Hyae-Jin Kim, Hyeon-Jeong Lee, Soeun Jeon, Jiseok Baik, Wangseok Do, Christine Kang, Yerin Kang","doi":"10.17085/apm.23161","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Spinal anesthesia-induced hypotension (SAH) frequently occurs in older patients, many of whom have mild left ventricular (LV) diastolic dysfunction, often asymptomatic at rest. This study investigated the association between preoperative echocardiographic measurements and SAH in older patients with mild LV diastolic dysfunction.</p><p><strong>Methods: </strong>We conducted a retrospective observational study using data from electronic medical records. The patients ≥ 65 years old who underwent spinal anesthesia for urologic surgery between January 2016 and December 2017 and whose preoperative echocardiography within 6 months before surgery revealed grade I LV diastolic dysfunction were recruited. SAH was investigated using the anesthesia records. Logistic regression and receiver operating characteristic (ROC) curve analyses were performed.</p><p><strong>Results: </strong>A total of 163 patients were analyzed. SAH and significant SAH developed in 55 (33.7%) patients. The mitral inflow E velocity was an independent risk factor for SAH (odds ratio [OR], 0.886; 95% confidence interval [CI], 0.845-0.929; P < 0.001). The area under the ROC curve for mitral inflow E velocity to predict SAH was 0.819 (95% CI, 0.752-0.875; P < 0.001). If mitral inflow E velocity was ≤ 60 cm/s, SAH was predicted with a sensitivity of 83.6% and specificity of 70.4%.</p><p><strong>Conclusions: </strong>The preoperative mitral inflow E velocity demonstrated the greatest predictability of SAH in older patients with mild LV diastolic dysfunction. This may assist in identifying patients at high risk of SAH and guiding preventive strategies in the future.</p>","PeriodicalId":101360,"journal":{"name":"Anesthesia and pain medicine","volume":"19 2","pages":"134-143"},"PeriodicalIF":3.2000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11089297/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.23161","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Spinal anesthesia-induced hypotension (SAH) frequently occurs in older patients, many of whom have mild left ventricular (LV) diastolic dysfunction, often asymptomatic at rest. This study investigated the association between preoperative echocardiographic measurements and SAH in older patients with mild LV diastolic dysfunction.
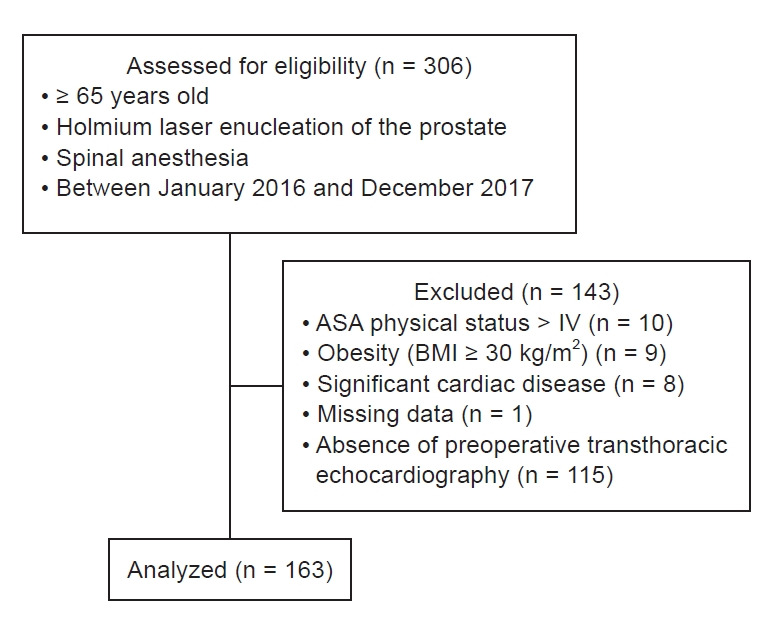
Methods: We conducted a retrospective observational study using data from electronic medical records. The patients ≥ 65 years old who underwent spinal anesthesia for urologic surgery between January 2016 and December 2017 and whose preoperative echocardiography within 6 months before surgery revealed grade I LV diastolic dysfunction were recruited. SAH was investigated using the anesthesia records. Logistic regression and receiver operating characteristic (ROC) curve analyses were performed.
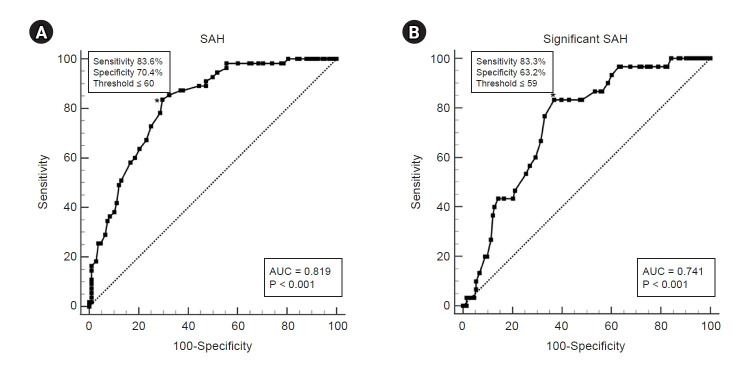
Results: A total of 163 patients were analyzed. SAH and significant SAH developed in 55 (33.7%) patients. The mitral inflow E velocity was an independent risk factor for SAH (odds ratio [OR], 0.886; 95% confidence interval [CI], 0.845-0.929; P < 0.001). The area under the ROC curve for mitral inflow E velocity to predict SAH was 0.819 (95% CI, 0.752-0.875; P < 0.001). If mitral inflow E velocity was ≤ 60 cm/s, SAH was predicted with a sensitivity of 83.6% and specificity of 70.4%.
Conclusions: The preoperative mitral inflow E velocity demonstrated the greatest predictability of SAH in older patients with mild LV diastolic dysfunction. This may assist in identifying patients at high risk of SAH and guiding preventive strategies in the future.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
