Santiago Gabardo, María Valencia-Mora, Ismael Coifman, Emilio Calvo
{"title":"Surgical anatomical landmarks for arthroscopic repair of subscapularis tendon tears.","authors":"Santiago Gabardo, María Valencia-Mora, Ismael Coifman, Emilio Calvo","doi":"10.5397/cise.2023.01165","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Subscapularis repair has recently garnered significant interest. A thorough understanding of the tendon's anatomy is essential for precise and safe repair. Our objectives were to describe the anatomy of the subscapularis insertion, define its landmarks, and analyze nearby structures to guide arthroscopic repair.</p><p><strong>Methods: </strong>We conducted an anatomical study, dissecting 12 shoulders. We evaluated the distance from the footprint to the axillary nerve, the dimensions, and shape of the footprint, and its relationship with the humeral cartilage.</p><p><strong>Results: </strong>The distance to the axillary nerve was 32 mm (standard deviation [SD], 3.7 mm). The craniocaudal length of the footprint was 37.3 mm (SD, 4.6 mm). Its largest mediolateral thickness was 16 mm (SD, 2.2 mm), wider at the top and narrower distally. The distance between the footprint and the cartilage varied, being 3.2 mm (SD, 1.2 mm) in the upper part, 5.4 mm (SD, 1.8 mm) in the medium, and 15.9 mm (SD, 2.9 mm) in the lower part.</p><p><strong>Conclusions: </strong>When performing a repair of the subscapularis tendon, the distance to the cartilage should be carefully evaluated as it varies proximally to distally, and the shape of the footprint (wider proximally, tapered distally) should be considered for implant positioning. The distance to the axillary nerve is approximately 30 mm. Anterior visualization guarantees direct control of all landmarks and allows accurate implant positioning with safe tendon release. Level of evidence: IV.</p>","PeriodicalId":33981,"journal":{"name":"Clinics in Shoulder and Elbow","volume":" ","pages":"272-277"},"PeriodicalIF":1.7000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11393444/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics in Shoulder and Elbow","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5397/cise.2023.01165","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
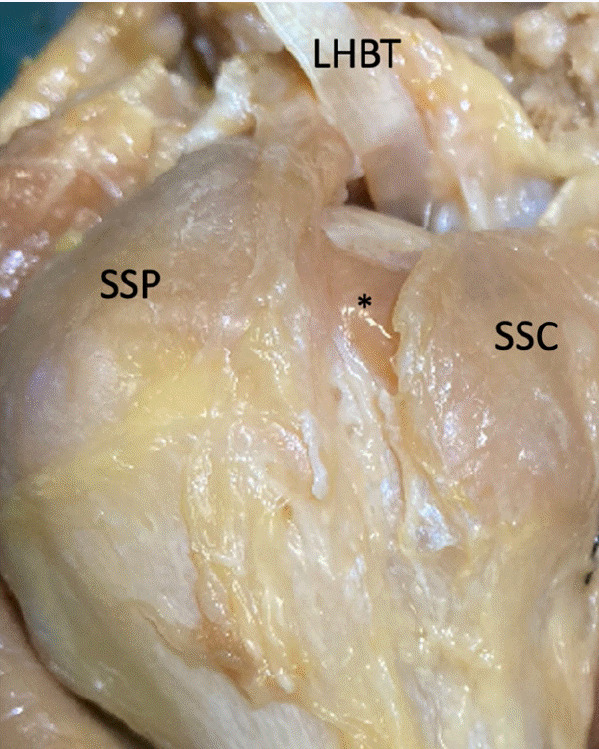
Background: Subscapularis repair has recently garnered significant interest. A thorough understanding of the tendon's anatomy is essential for precise and safe repair. Our objectives were to describe the anatomy of the subscapularis insertion, define its landmarks, and analyze nearby structures to guide arthroscopic repair.
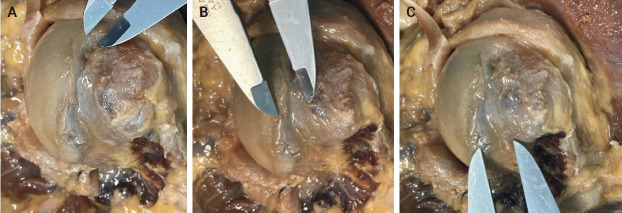
Methods: We conducted an anatomical study, dissecting 12 shoulders. We evaluated the distance from the footprint to the axillary nerve, the dimensions, and shape of the footprint, and its relationship with the humeral cartilage.
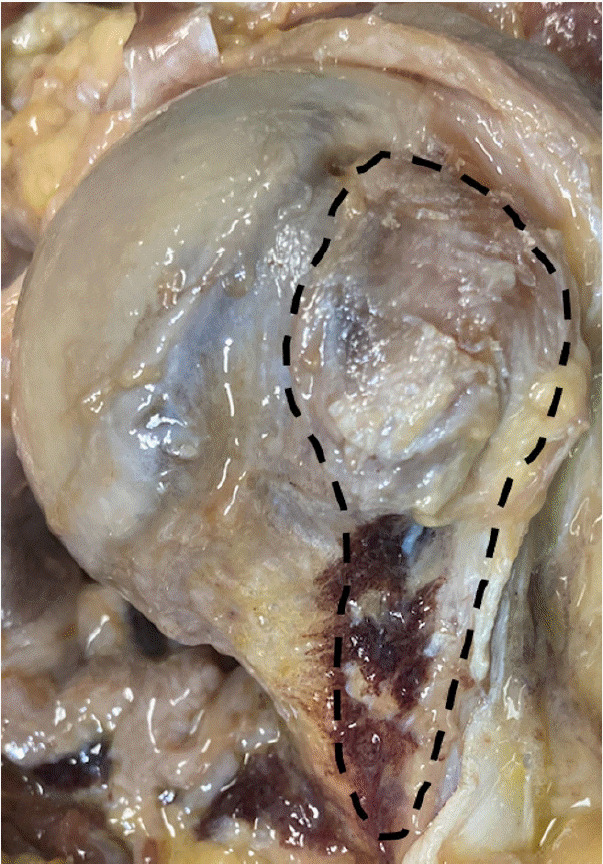
Results: The distance to the axillary nerve was 32 mm (standard deviation [SD], 3.7 mm). The craniocaudal length of the footprint was 37.3 mm (SD, 4.6 mm). Its largest mediolateral thickness was 16 mm (SD, 2.2 mm), wider at the top and narrower distally. The distance between the footprint and the cartilage varied, being 3.2 mm (SD, 1.2 mm) in the upper part, 5.4 mm (SD, 1.8 mm) in the medium, and 15.9 mm (SD, 2.9 mm) in the lower part.
Conclusions: When performing a repair of the subscapularis tendon, the distance to the cartilage should be carefully evaluated as it varies proximally to distally, and the shape of the footprint (wider proximally, tapered distally) should be considered for implant positioning. The distance to the axillary nerve is approximately 30 mm. Anterior visualization guarantees direct control of all landmarks and allows accurate implant positioning with safe tendon release. Level of evidence: IV.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
