{"title":"Pneumocephalus resulting from traumatic pneumothorax and brachial plexus avulsion","authors":"Naoki Date, Hiroshi Hamakawa, Ichiro Sakanoue, Tomoki Saito, Yutaka Takahashi","doi":"10.1002/ams2.956","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Traumatic pneumocephalus is commonly encountered after basal skull fractures and rarely associated with blunt chest trauma. Here, we report a case of pneumocephalus caused by traumatic pneumothorax and brachial plexus avulsion.</p>\n </section>\n \n <section>\n \n <h3> Case Presentation</h3>\n \n <p>A 20-year-old male was admitted to our hospital following a motorcycle accident with complete paralysis of the right upper limb. 2 days later, follow-up computed tomography revealed a slight right pneumothorax, pneumomediastinum around the neck, and intracranial air without skull fracture. Air migrates into the subarachnoid space through a dural tear caused by a brachial plexus avulsion. The pneumocephalus immediately improved after the insertion of a chest drain.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Pneumothorax combined with brachial plexus avulsion could lead to pneumocephalus. Immediate chest drainage might be the best way to stop the migration of air; however, care should be taken to not worsen cerebrospinal fluid leakage.</p>\n </section>\n </div>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"11 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.956","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.956","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Traumatic pneumocephalus is commonly encountered after basal skull fractures and rarely associated with blunt chest trauma. Here, we report a case of pneumocephalus caused by traumatic pneumothorax and brachial plexus avulsion.
Case Presentation
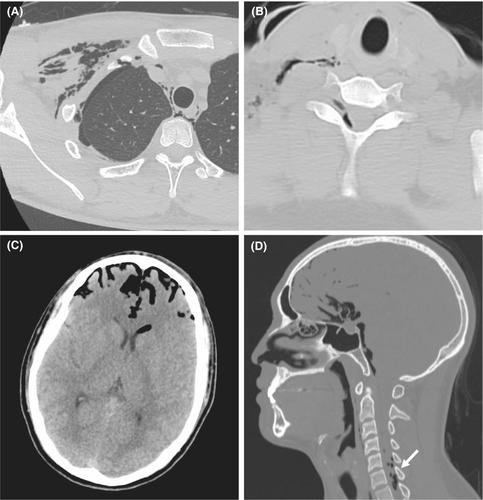
A 20-year-old male was admitted to our hospital following a motorcycle accident with complete paralysis of the right upper limb. 2 days later, follow-up computed tomography revealed a slight right pneumothorax, pneumomediastinum around the neck, and intracranial air without skull fracture. Air migrates into the subarachnoid space through a dural tear caused by a brachial plexus avulsion. The pneumocephalus immediately improved after the insertion of a chest drain.
Conclusion
Pneumothorax combined with brachial plexus avulsion could lead to pneumocephalus. Immediate chest drainage might be the best way to stop the migration of air; however, care should be taken to not worsen cerebrospinal fluid leakage.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
