Teodora Biciusca, Leon D Gruenewald, Simon S Martin, Jennifer Gotta, Scherwin Mahmoudi, Katrin Eichler, Christian Booz, Christian Salbach, Matthias Müller-Hennessen, Moritz Biener, Mustafa Yildirim, Barbara Milles, Christof M Sommer, Thomas J Vogl, Evangelos Giannitsis, Vitali Koch
{"title":"Optimizing resource allocation: Cost-effectiveness of specified D-dimer cut-offs in cancer patients with suspected venous thromboembolism.","authors":"Teodora Biciusca, Leon D Gruenewald, Simon S Martin, Jennifer Gotta, Scherwin Mahmoudi, Katrin Eichler, Christian Booz, Christian Salbach, Matthias Müller-Hennessen, Moritz Biener, Mustafa Yildirim, Barbara Milles, Christof M Sommer, Thomas J Vogl, Evangelos Giannitsis, Vitali Koch","doi":"10.1007/s11239-024-03000-2","DOIUrl":null,"url":null,"abstract":"<p><p>An accurate diagnosis of venous thromboembolism (VTE) is crucial, given the potential for high mortality in undetected cases. Strategic D-dimer testing may aid in identifying low-risk patients, preventing overdiagnosis and reducing imaging costs. We conducted a retrospective, comparative analysis to assess the potential cost savings that could be achieved by adopting different approaches to determine the most effective D-dimer cut-off value in cancer patients with suspected VTE, compared to the commonly used rule-out cut-off level of 0.5 mg/L. The study included 526 patients (median age 65, IQR 55-75) with a confirmed cancer diagnosis who underwent D-dimer testing. Among these patients, the VTE prevalence was 29% (n = 152). Each diagnostic strategy's sensitivity, specificity, negative likelihood ratio (NLR), as well as positive likelihood ratio (PLR), and the proportion of patients exhibiting a negative D-dimer test result, were calculated. The diagnostic strategy that demonstrated the best balance between specificity, sensitivity, NLR, and PLR, utilized an inverse age-specific cut-off level for D-dimer [0.5 + (66-age) × 0.01 mg/L]. This method yielded a PLR of 2.9 at a very low NLR for the exclusion of VTE. We observed a significant cost reduction of 4.6% and 1.0% for PE and DVT, respectively. The utilization of an age-adjusted cut-off [patient's age × 0.01 mg/L] resulted in the highest cost savings, reaching 8.1% for PE and 3.4% for DVT. Using specified D-dimer cut-offs in the diagnosis of VTE could improve economics, considering the limited occurrence of confirmed cases among patients with suspected VTE.</p>","PeriodicalId":17546,"journal":{"name":"Journal of Thrombosis and Thrombolysis","volume":" ","pages":"996-1007"},"PeriodicalIF":2.2000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11315745/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thrombosis and Thrombolysis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11239-024-03000-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/18 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
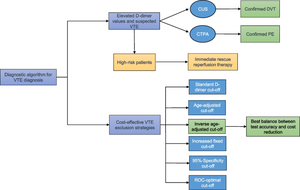
An accurate diagnosis of venous thromboembolism (VTE) is crucial, given the potential for high mortality in undetected cases. Strategic D-dimer testing may aid in identifying low-risk patients, preventing overdiagnosis and reducing imaging costs. We conducted a retrospective, comparative analysis to assess the potential cost savings that could be achieved by adopting different approaches to determine the most effective D-dimer cut-off value in cancer patients with suspected VTE, compared to the commonly used rule-out cut-off level of 0.5 mg/L. The study included 526 patients (median age 65, IQR 55-75) with a confirmed cancer diagnosis who underwent D-dimer testing. Among these patients, the VTE prevalence was 29% (n = 152). Each diagnostic strategy's sensitivity, specificity, negative likelihood ratio (NLR), as well as positive likelihood ratio (PLR), and the proportion of patients exhibiting a negative D-dimer test result, were calculated. The diagnostic strategy that demonstrated the best balance between specificity, sensitivity, NLR, and PLR, utilized an inverse age-specific cut-off level for D-dimer [0.5 + (66-age) × 0.01 mg/L]. This method yielded a PLR of 2.9 at a very low NLR for the exclusion of VTE. We observed a significant cost reduction of 4.6% and 1.0% for PE and DVT, respectively. The utilization of an age-adjusted cut-off [patient's age × 0.01 mg/L] resulted in the highest cost savings, reaching 8.1% for PE and 3.4% for DVT. Using specified D-dimer cut-offs in the diagnosis of VTE could improve economics, considering the limited occurrence of confirmed cases among patients with suspected VTE.
期刊介绍:
The Journal of Thrombosis and Thrombolysis is a long-awaited resource for contemporary cardiologists, hematologists, vascular medicine specialists and clinician-scientists actively involved in treatment decisions and clinical investigation of thrombotic disorders involving the cardiovascular and cerebrovascular systems. The principal focus of the Journal centers on the pathobiology of thrombosis and vascular disorders and the use of anticoagulants, platelet antagonists, cell-based therapies and interventions in scientific investigation, clinical-translational research and patient care.
The Journal will publish original work which emphasizes the interface between fundamental scientific principles and clinical investigation, stimulating an interdisciplinary and scholarly dialogue in thrombosis and vascular science. Published works will also define platforms for translational research, drug development, clinical trials and patient-directed applications. The Journal of Thrombosis and Thrombolysis'' integrated format will expand the reader''s knowledge base and provide important insights for both the investigation and direct clinical application of the most rapidly growing fields in medicine-thrombosis and vascular science.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
