Development and validation of a nomogram to predict postoperative delirium in older patients after major abdominal surgery: a retrospective case-control study.
{"title":"Development and validation of a nomogram to predict postoperative delirium in older patients after major abdominal surgery: a retrospective case-control study.","authors":"Yun-Gen Luo, Xiao-Dong Wu, Yu-Xiang Song, Xiao-Lin Wang, Kai Liu, Chun-Ting Shi, Zi-Lin Wang, Yu-Long Ma, Hao Li, Yan-Hong Liu, Wei-Dong Mi, Jing-Sheng Lou, Jiang-Bei Cao","doi":"10.1186/s13741-024-00399-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postoperative delirium is a common complication in older patients, with poor long-term outcomes. This study aimed to investigate risk factors and develop a predictive model for postoperative delirium in older patients after major abdominal surgery.</p><p><strong>Methods: </strong>This study retrospectively recruited 7577 patients aged ≥ 65 years who underwent major abdominal surgery between January 2014 and December 2018 in a single hospital in Beijing, China. Patients were divided into a training cohort (n = 5303) and a validation cohort (n = 2224) for univariate and multivariate logistic regression analyses and to build a nomogram. Data were collected for 43 perioperative variables, including demographics, medical history, preoperative laboratory results, imaging, and anesthesia information.</p><p><strong>Results: </strong>Age, chronic obstructive pulmonary disease, white blood cell count, glucose, total protein, creatinine, emergency surgery, and anesthesia time were associated with postoperative delirium in multivariate analysis. We developed a nomogram based on the above 8 variables. The nomogram achieved areas under the curve of 0.731 and 0.735 for the training and validation cohorts, respectively. The discriminatory ability of the nomogram was further assessed by dividing the cases into three risk groups (low-risk, nomogram score < 175; medium-risk, nomogram score 175~199; high-risk, nomogram score > 199; P < 0.001). Decision curve analysis revealed that the nomogram provided a good net clinical benefit.</p><p><strong>Conclusions: </strong>We developed a nomogram that could predict postoperative delirium with high accuracy and stability in older patients after major abdominal surgery.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"13 1","pages":"41"},"PeriodicalIF":2.1000,"publicationDate":"2024-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11100071/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-024-00399-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Postoperative delirium is a common complication in older patients, with poor long-term outcomes. This study aimed to investigate risk factors and develop a predictive model for postoperative delirium in older patients after major abdominal surgery.
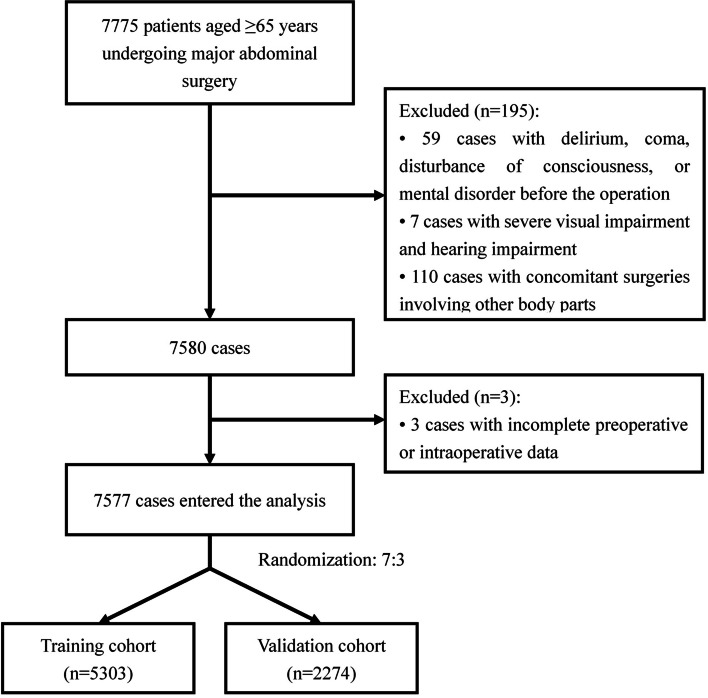
Methods: This study retrospectively recruited 7577 patients aged ≥ 65 years who underwent major abdominal surgery between January 2014 and December 2018 in a single hospital in Beijing, China. Patients were divided into a training cohort (n = 5303) and a validation cohort (n = 2224) for univariate and multivariate logistic regression analyses and to build a nomogram. Data were collected for 43 perioperative variables, including demographics, medical history, preoperative laboratory results, imaging, and anesthesia information.
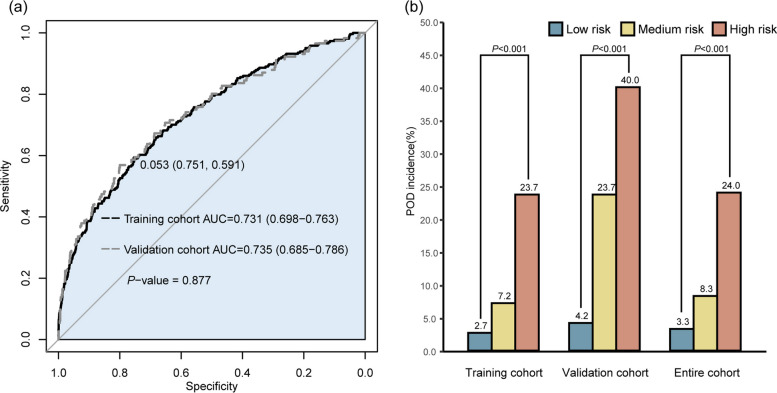
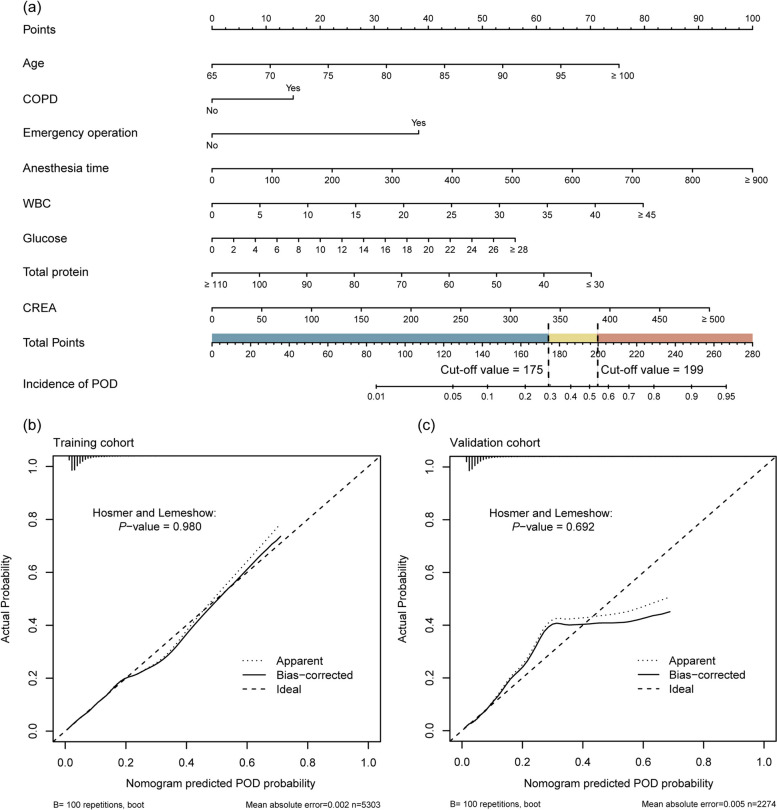
Results: Age, chronic obstructive pulmonary disease, white blood cell count, glucose, total protein, creatinine, emergency surgery, and anesthesia time were associated with postoperative delirium in multivariate analysis. We developed a nomogram based on the above 8 variables. The nomogram achieved areas under the curve of 0.731 and 0.735 for the training and validation cohorts, respectively. The discriminatory ability of the nomogram was further assessed by dividing the cases into three risk groups (low-risk, nomogram score < 175; medium-risk, nomogram score 175~199; high-risk, nomogram score > 199; P < 0.001). Decision curve analysis revealed that the nomogram provided a good net clinical benefit.
Conclusions: We developed a nomogram that could predict postoperative delirium with high accuracy and stability in older patients after major abdominal surgery.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
