Andrew A Lawson, Paul Tannous, Christina Laternser, Karl Migally
{"title":"The Estimated Fick Method Systematically Over-Estimates Cardiac Index Compared to Thermodilution in Children.","authors":"Andrew A Lawson, Paul Tannous, Christina Laternser, Karl Migally","doi":"10.1007/s00246-024-03491-z","DOIUrl":null,"url":null,"abstract":"<p><p>Cardiac index (CI) may be derived from the Fick method, using measured or estimated oxygen consumption (VO<sub>2</sub>), or from thermodilution. In children, LaFarge VO<sub>2</sub> estimates correlate poorly with measured VO<sub>2</sub> values. In a large adult cohort, there was only modest correlation between estimated Fick CI (eFick CI) and thermodilution CI (TDCI). We evaluated the extent of agreement between eFick CI using LaFarge estimates of VO<sub>2</sub> and TDCI in a pediatric cohort. A retrospective, single-center chart review of patients 3-18 years of age who underwent cardiac catheterization with documented eFick CI and TDCI from 2004 to 2020 included 201 catheterizations from 161 unique patients. The mean patient age at catheterization was 12.2y (SD 4.4y). The most frequent diagnosis was cardiomyopathy, followed by congenital heart disease and pulmonary hypertension. TDCI and eFick CI differed by > 20% in 49% of catheterizations. eFick CI systematically exceeded TDCI by a mean percentage difference of 24% (SD 31%). Higher mean CI ((eFick CI + TDCI)/2) and older age were predictive of greater percent difference between eFick CI and TDCI. For each increase in mean CI by 1.0 L/min/m<sup>2</sup>, the expected percent difference in CI increased by 9.9% (p < 0.001). In pediatric patients undergoing cardiac catheterization, eFick CI with LaFarge VO<sub>2</sub> systematically exceeds TDCI. The difference between methods is frequently > 20%, which may have clinically significant implications. Discrepancies between eFick CI and TDCI increase at higher mean CI.</p>","PeriodicalId":19814,"journal":{"name":"Pediatric Cardiology","volume":" ","pages":"713-718"},"PeriodicalIF":1.4000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00246-024-03491-z","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
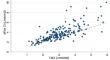
Cardiac index (CI) may be derived from the Fick method, using measured or estimated oxygen consumption (VO2), or from thermodilution. In children, LaFarge VO2 estimates correlate poorly with measured VO2 values. In a large adult cohort, there was only modest correlation between estimated Fick CI (eFick CI) and thermodilution CI (TDCI). We evaluated the extent of agreement between eFick CI using LaFarge estimates of VO2 and TDCI in a pediatric cohort. A retrospective, single-center chart review of patients 3-18 years of age who underwent cardiac catheterization with documented eFick CI and TDCI from 2004 to 2020 included 201 catheterizations from 161 unique patients. The mean patient age at catheterization was 12.2y (SD 4.4y). The most frequent diagnosis was cardiomyopathy, followed by congenital heart disease and pulmonary hypertension. TDCI and eFick CI differed by > 20% in 49% of catheterizations. eFick CI systematically exceeded TDCI by a mean percentage difference of 24% (SD 31%). Higher mean CI ((eFick CI + TDCI)/2) and older age were predictive of greater percent difference between eFick CI and TDCI. For each increase in mean CI by 1.0 L/min/m2, the expected percent difference in CI increased by 9.9% (p < 0.001). In pediatric patients undergoing cardiac catheterization, eFick CI with LaFarge VO2 systematically exceeds TDCI. The difference between methods is frequently > 20%, which may have clinically significant implications. Discrepancies between eFick CI and TDCI increase at higher mean CI.
期刊介绍:
The editor of Pediatric Cardiology welcomes original manuscripts concerning all aspects of heart disease in infants, children, and adolescents, including embryology and anatomy, physiology and pharmacology, biochemistry, pathology, genetics, radiology, clinical aspects, investigative cardiology, electrophysiology and echocardiography, and cardiac surgery. Articles which may include original articles, review articles, letters to the editor etc., must be written in English and must be submitted solely to Pediatric Cardiology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
