Lisa K. Stamp, Anne Horne, Borislav Mihov, Jill Drake, Janine Haslett, Peter Chapman, Christopher Frampton, Nicola Dalbeth
{"title":"Predicting Gout Flares in People Starting Allopurinol Using the Start-Low Go-Slow Dose Escalation Strategy","authors":"Lisa K. Stamp, Anne Horne, Borislav Mihov, Jill Drake, Janine Haslett, Peter Chapman, Christopher Frampton, Nicola Dalbeth","doi":"10.1002/acr.25376","DOIUrl":null,"url":null,"abstract":"<div>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>The study objective was to determine predictors of gout flare when commencing allopurinol using the “start-low go-slow” dose escalation strategy.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A post hoc analysis of a 12-month double-blind placebo-controlled noninferiority trial with participants randomized 1:1 to colchicine 0.5 mg daily or placebo for the first six months was undertaken. Multivariate logistic regression models were used to identify independent predictors of gout flares in the first and last six months of the trial.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Multivariable analysis revealed a significant association between risk of a gout flare in the first six months and flare in the month before starting allopurinol (odds ratio [OR] 2.65, 95% confidence interval [CI] 1.36–5.17) and allopurinol 100 mg starting dose (OR 3.21, 95% CI 1.41–7.27). The predictors of any gout flares in the last six months of the trial, after stopping colchicine or placebo, were having received colchicine (OR 2.95, 95% CI 1.48–5.86), at least one flare in the month before stopping study drug (OR 5.39, 95% CI 2.21–13.15), and serum urate ≥0.36 mmol/L at month 6 (OR 2.85, 95% CI 1.14–7.12).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Anti-inflammatory prophylaxis when starting allopurinol using the “start-low go-slow” dose escalation strategy may be best targeted at those who have had a gout flare in the month before starting allopurinol and are commencing allopurinol 100 mg daily. For those with ongoing gout flares during the first six months of starting allopurinol who have not yet achieved serum urate target, a longer period of prophylaxis may be required.</p>\n </section>\n </div>","PeriodicalId":8406,"journal":{"name":"Arthritis Care & Research","volume":"76 10","pages":"1371-1378"},"PeriodicalIF":3.3000,"publicationDate":"2024-05-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/acr.25376","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthritis Care & Research","FirstCategoryId":"3","ListUrlMain":"https://acrjournals.onlinelibrary.wiley.com/doi/10.1002/acr.25376","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
The study objective was to determine predictors of gout flare when commencing allopurinol using the “start-low go-slow” dose escalation strategy.
Methods
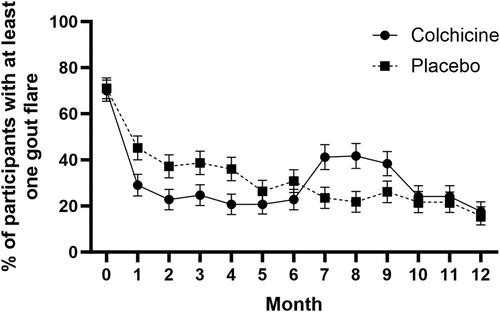
A post hoc analysis of a 12-month double-blind placebo-controlled noninferiority trial with participants randomized 1:1 to colchicine 0.5 mg daily or placebo for the first six months was undertaken. Multivariate logistic regression models were used to identify independent predictors of gout flares in the first and last six months of the trial.
Results
Multivariable analysis revealed a significant association between risk of a gout flare in the first six months and flare in the month before starting allopurinol (odds ratio [OR] 2.65, 95% confidence interval [CI] 1.36–5.17) and allopurinol 100 mg starting dose (OR 3.21, 95% CI 1.41–7.27). The predictors of any gout flares in the last six months of the trial, after stopping colchicine or placebo, were having received colchicine (OR 2.95, 95% CI 1.48–5.86), at least one flare in the month before stopping study drug (OR 5.39, 95% CI 2.21–13.15), and serum urate ≥0.36 mmol/L at month 6 (OR 2.85, 95% CI 1.14–7.12).
Conclusion
Anti-inflammatory prophylaxis when starting allopurinol using the “start-low go-slow” dose escalation strategy may be best targeted at those who have had a gout flare in the month before starting allopurinol and are commencing allopurinol 100 mg daily. For those with ongoing gout flares during the first six months of starting allopurinol who have not yet achieved serum urate target, a longer period of prophylaxis may be required.
期刊介绍:
Arthritis Care & Research, an official journal of the American College of Rheumatology and the Association of Rheumatology Health Professionals (a division of the College), is a peer-reviewed publication that publishes original research, review articles, and editorials that promote excellence in the clinical practice of rheumatology. Relevant to the care of individuals with rheumatic diseases, major topics are evidence-based practice studies, clinical problems, practice guidelines, educational, social, and public health issues, health economics, health care policy, and future trends in rheumatology practice.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
