Tarana Gupta, Ashank Goel, Naveen Ranga, Sandeep K Goyal
{"title":"Comparison of intravenous terlipressin infusion versus bolus in patients with acute-on-chronic liver failure-acute kidney injury - an open label RCT.","authors":"Tarana Gupta, Ashank Goel, Naveen Ranga, Sandeep K Goyal","doi":"10.5114/ceh.2023.132813","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim of the study: </strong>Despite having ample literature in hepatorenal syndrome-acute kidney injury (HRS-AKI) in decompensated cirrhosis patients, there is a scarcity of data on acute-on-chronic liver failure-acute kidney injury (ACLF-AKI). We compared terlipressin infusion with bolus in ACLF-AKI patients.</p><p><strong>Material and methods: </strong>Patients with ACLF (as per the CANONIC study) were screened for AKI as per the 2015 ICA-AKI criteria. If after 48 h of volume expansion with albumin, serum creatinine (sCr) did not improve, patients were randomized into two groups: Terli-infusion (Terli-I) 2 mg/day and Terli-bolus (Terli-B) 1 mg q6h. If sCr did not decrease < 25% of pretreatment value after 48 h, the terlipressin dose was increased to a maximum of 12 mg/day. The primary outcome was taken as regression (full or partial response), stable/no response and progression of AKI to higher stages and secondary outcomes were taken as 28-day and 90-day mortality.</p><p><strong>Results: </strong>After screening 136 patients with ACLF-AKI, Terli-I (<i>n</i> = 50) and Terli-B (<i>n</i> = 50) with mean sCr 2.4 and 2.1 mg/dl respectively were enrolled. The regression of AKI (full response 37 vs. 27, partial response 3 vs. 9, <i>p</i> = 0.5), stable (2 vs. 5, <i>p</i> = 0.6), progression of AKI (8 vs. 7, <i>p</i> = 0.2) were present in Terli-I and Terli-B respectively. No significant difference was found in 28-and 90-day mortality. In Terli-B, mean terlipressin dose was 8 vs. 4 mg, <i>p</i> < 0.008 with more side effects, 15 vs. 0, <i>p</i> < 0.01 than Terli-I respectively.</p><p><strong>Conclusions: </strong>Terlipressin infusion is more effective than bolus doses in regression of acute kidney injury and better tolerated in acute-on-chronic liver failure-AKI patients.</p>","PeriodicalId":10281,"journal":{"name":"Clinical and Experimental Hepatology","volume":"9 4","pages":"351-358"},"PeriodicalIF":1.7000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11103809/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/ceh.2023.132813","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/5 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Aim of the study: Despite having ample literature in hepatorenal syndrome-acute kidney injury (HRS-AKI) in decompensated cirrhosis patients, there is a scarcity of data on acute-on-chronic liver failure-acute kidney injury (ACLF-AKI). We compared terlipressin infusion with bolus in ACLF-AKI patients.
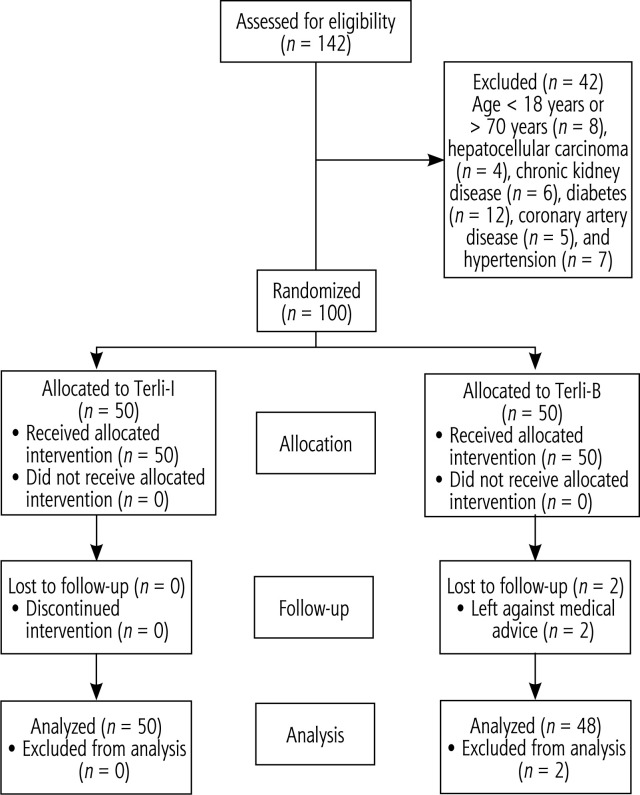
Material and methods: Patients with ACLF (as per the CANONIC study) were screened for AKI as per the 2015 ICA-AKI criteria. If after 48 h of volume expansion with albumin, serum creatinine (sCr) did not improve, patients were randomized into two groups: Terli-infusion (Terli-I) 2 mg/day and Terli-bolus (Terli-B) 1 mg q6h. If sCr did not decrease < 25% of pretreatment value after 48 h, the terlipressin dose was increased to a maximum of 12 mg/day. The primary outcome was taken as regression (full or partial response), stable/no response and progression of AKI to higher stages and secondary outcomes were taken as 28-day and 90-day mortality.
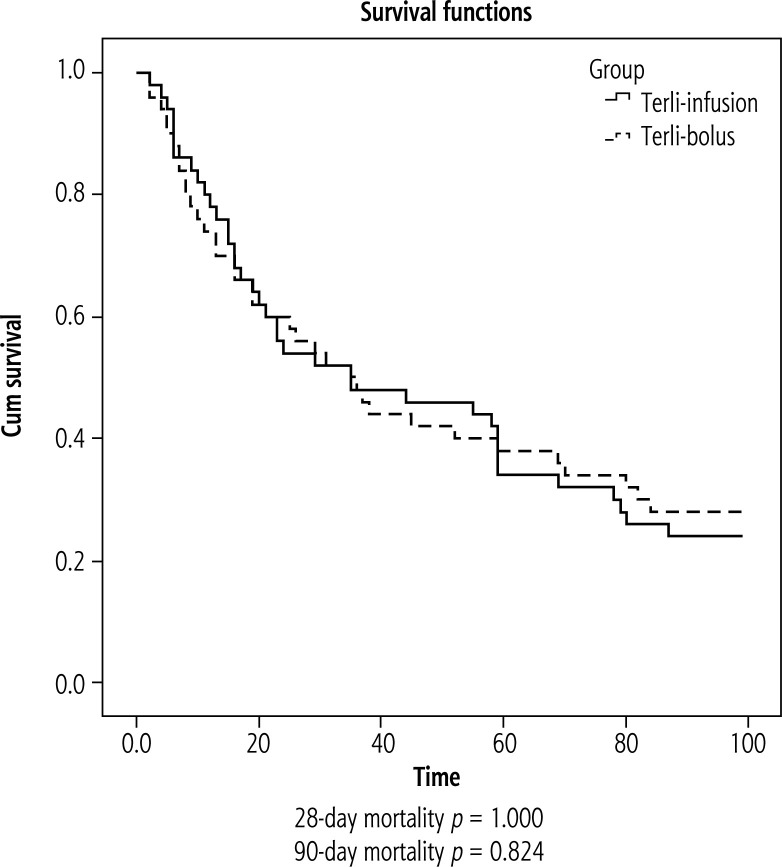
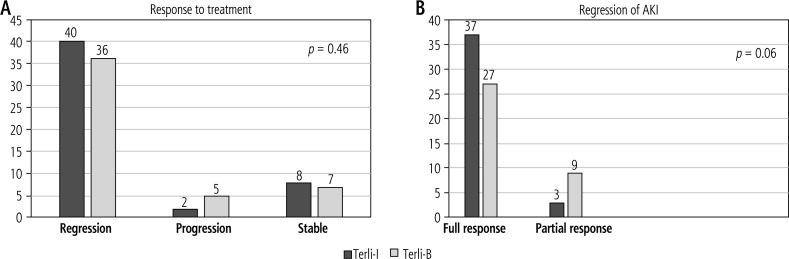
Results: After screening 136 patients with ACLF-AKI, Terli-I (n = 50) and Terli-B (n = 50) with mean sCr 2.4 and 2.1 mg/dl respectively were enrolled. The regression of AKI (full response 37 vs. 27, partial response 3 vs. 9, p = 0.5), stable (2 vs. 5, p = 0.6), progression of AKI (8 vs. 7, p = 0.2) were present in Terli-I and Terli-B respectively. No significant difference was found in 28-and 90-day mortality. In Terli-B, mean terlipressin dose was 8 vs. 4 mg, p < 0.008 with more side effects, 15 vs. 0, p < 0.01 than Terli-I respectively.
Conclusions: Terlipressin infusion is more effective than bolus doses in regression of acute kidney injury and better tolerated in acute-on-chronic liver failure-AKI patients.
期刊介绍:
Clinical and Experimental Hepatology – quarterly of the Polish Association for Study of Liver – is a scientific and educational, peer-reviewed journal publishing original and review papers describing clinical and basic investigations in the field of hepatology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
