Anthony Kerbage, Tarek Nammour, Hani Tamim, Maha Makki, Yasser H Shaib, Ala I Sharara, Fadi Mourad, Jana G Hashash, Lara El Jamal, Don C Rockey, Kassem Barada
{"title":"Impact of blood transfusion on mortality and rebleeding in gastrointestinal bleeding: an 8-year cohort from a tertiary care center.","authors":"Anthony Kerbage, Tarek Nammour, Hani Tamim, Maha Makki, Yasser H Shaib, Ala I Sharara, Fadi Mourad, Jana G Hashash, Lara El Jamal, Don C Rockey, Kassem Barada","doi":"10.20524/aog.2024.0877","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of this study was to investigate the impact of blood transfusion (BT) on mortality and rebleeding in patients with gastrointestinal bleeding (GIB) and whether BT at a threshold of ≤7 g/dL may improve these outcomes.</p><p><strong>Methods: </strong>A prospective study was conducted in patients admitted with GIB between 2013 and 2021. Antithrombotic (AT) use and clinical outcomes were compared between transfused and non-transfused patients, and between those transfused at a threshold of ≤7 vs. >7 g/dL. Multivariate analysis was performed to identify predictors of mortality and rebleeding.</p><p><strong>Results: </strong>A total of 667 patients, including 383 transfused, were followed up for a median of 56 months. Predictors of end-of-follow-up mortality included: age-adjusted Charlson Comorbidity Index, stigmata of recent hemorrhage (SRH), and being on anticoagulants only upon presentation (P=0.026). SRH was a predictor of end-of-follow-up rebleeding, while having been on only antiplatelet therapy (AP) upon presentation was protective (P<0.001). BT was not associated with mortality or rebleeding at 1 month or end of follow up. Among transfused patients, being discharged only on AP protected against mortality (P=0.044). BT at >7 g/dL did not affect the risk of short or long-term rebleeding or mortality compared to BT at ≤7 g/dL.</p><p><strong>Conclusions: </strong>Short- and long-term mortality and rebleeding in GIB were not affected by BT, nor by a transfusion threshold of ≤7 vs. >7 g/dL, but were affected by the use of AT. Further studies that account for AT use are needed to determine the best transfusion strategy in GIB.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 3","pages":"303-312"},"PeriodicalIF":2.7000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11107406/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0877","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The aim of this study was to investigate the impact of blood transfusion (BT) on mortality and rebleeding in patients with gastrointestinal bleeding (GIB) and whether BT at a threshold of ≤7 g/dL may improve these outcomes.
Methods: A prospective study was conducted in patients admitted with GIB between 2013 and 2021. Antithrombotic (AT) use and clinical outcomes were compared between transfused and non-transfused patients, and between those transfused at a threshold of ≤7 vs. >7 g/dL. Multivariate analysis was performed to identify predictors of mortality and rebleeding.
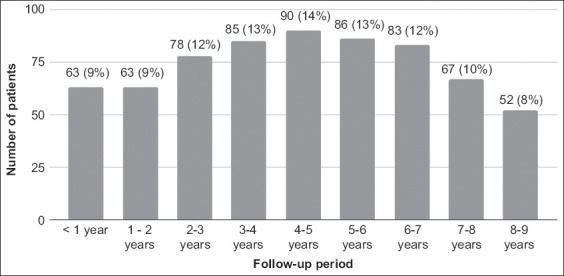
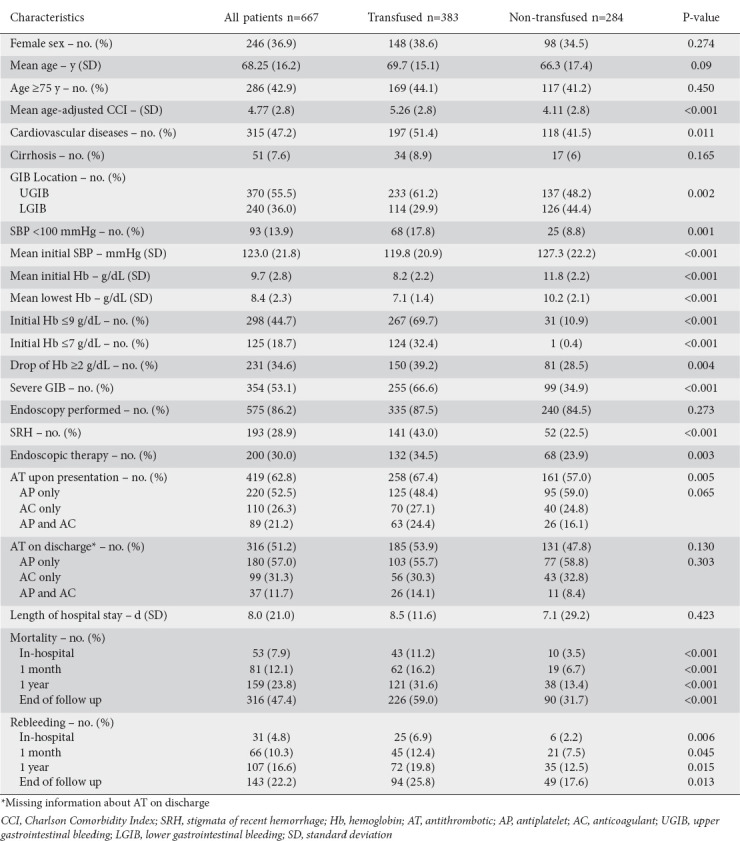
Results: A total of 667 patients, including 383 transfused, were followed up for a median of 56 months. Predictors of end-of-follow-up mortality included: age-adjusted Charlson Comorbidity Index, stigmata of recent hemorrhage (SRH), and being on anticoagulants only upon presentation (P=0.026). SRH was a predictor of end-of-follow-up rebleeding, while having been on only antiplatelet therapy (AP) upon presentation was protective (P<0.001). BT was not associated with mortality or rebleeding at 1 month or end of follow up. Among transfused patients, being discharged only on AP protected against mortality (P=0.044). BT at >7 g/dL did not affect the risk of short or long-term rebleeding or mortality compared to BT at ≤7 g/dL.
Conclusions: Short- and long-term mortality and rebleeding in GIB were not affected by BT, nor by a transfusion threshold of ≤7 vs. >7 g/dL, but were affected by the use of AT. Further studies that account for AT use are needed to determine the best transfusion strategy in GIB.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
