Chi Nguyen, Christopher L Crowe, Effie Kuti, Bonnie Donato, Rachel Djaraher, Leo Seman, Nancy Graeter, Thomas P Power, Rinku Mehra, Vincent J Willey
{"title":"Impact of Pre-existing Type 2 Diabetes Mellitus and Cardiovascular Disease on Healthcare Resource Utilization and Costs in Patients With COVID-19.","authors":"Chi Nguyen, Christopher L Crowe, Effie Kuti, Bonnie Donato, Rachel Djaraher, Leo Seman, Nancy Graeter, Thomas P Power, Rinku Mehra, Vincent J Willey","doi":"10.36469/001c.92368","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The economic burden associated with type 2 diabetes mellitus (T2DM) and concurrent cardiovascular disease (CVD) among patients with COVID-19 is unclear. <b>Objective:</b> We compared healthcare resource utilization (HCRU) and costs in patients with COVID-19 and T2DM and CVD (T2DM + CVD), T2DM only, or neither T2DM nor CVD (T2DM/CVD). <b>Methods:</b> A retrospective observational study in COVID-19 patients using data from the Healthcare Integrated Research Database (HIRD®) was conducted. Patients with COVID-19 were identified between March 1, 2020, and May 31, 2021, and followed from first diagnosis or positive lab test to the end of health plan enrollment, end of study period, or death. Patients were assigned one of 3 cohorts: pre-existing T2DM+CVD, T2DM only, or neither T2DM/CVD. Propensity score matching and multivariable analyses were performed to control for differences in baseline characteristics. Study outcomes included all-cause and COVID-19-related HCRU and costs. <b>Results:</b> In all, 321 232 COVID-19 patients were identified (21 651 with T2DM + CVD, 28 184 with T2DM only, and 271 397 with neither T2DM/CVD). After matching, 6967 patients were in each group. Before matching, 46.0% of patients in the T2DM + CVD cohort were hospitalized for any cause, compared with 18.0% in the T2DM-only cohort and 6.3% in the neither T2DM/CVD cohort; the corresponding values after matching were 34.2%, 26.0%, and 21.2%. The proportion of patients with emergency department visits, telehealth visits, or use of skilled nursing facilities was higher in patients with COVID-19 and T2DM + CVD compared with the other cohorts. Average all-cause costs during follow-up were <math><mn>12</mn><mrow><mo> </mo></mrow><mn>324</mn><mo>,</mo></math>7882, and $7277 per-patient-per-month after matching for patients with T2DM + CVD, T2DM-only, and neither T2DM/CVD, respectively. COVID-19-related costs contributed to 78%, 75%, and 64% of the overall costs, respectively. The multivariable model showed that per-patient-per-month all-cause costs for T2DM + CVD and T2DM-only were 54% and 21% higher, respectively, than those with neither T2DM/CVD after adjusting for residual confounding. <b>Conclusion:</b> HCRU and costs in patients were incrementally higher with COVID-19 and pre-existing T2DM + CVD compared with those with T2DM-only and neither T2DM/CVD, even after accounting for baseline differences between groups, confirming that pre-existing T2DM + CVD is associated with increased HCRU and costs in COVID-19 patients, highlighting the importance of proactive management.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"11 1","pages":"112-121"},"PeriodicalIF":2.3000,"publicationDate":"2024-04-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11110887/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.92368","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
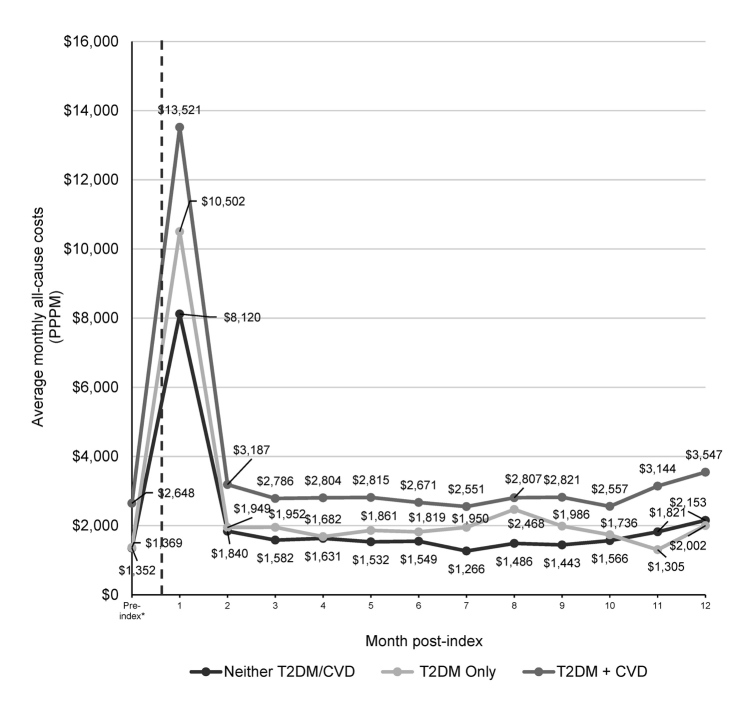
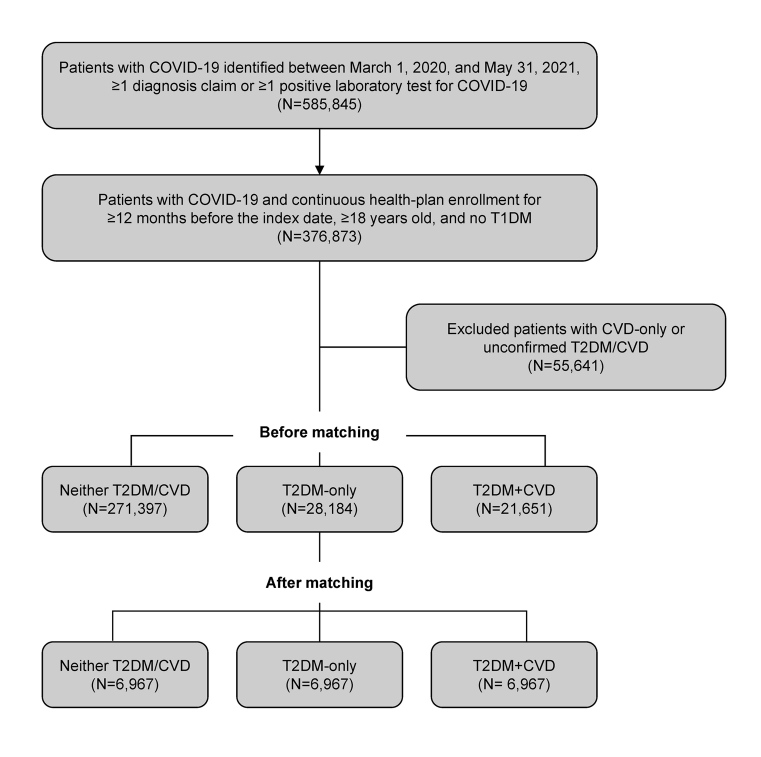
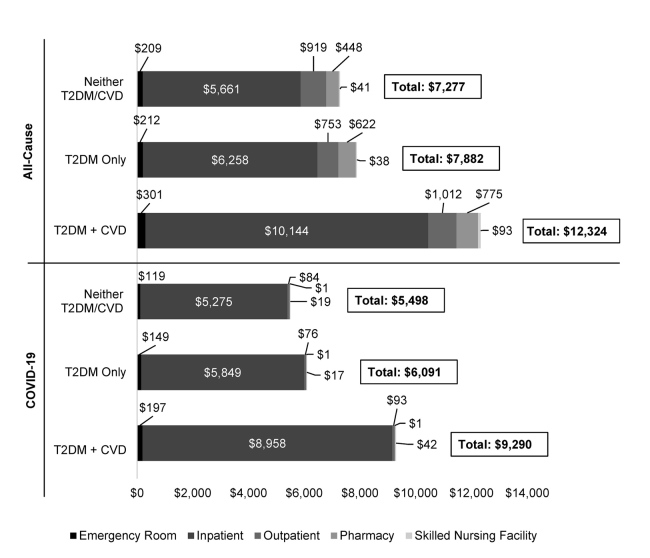
Background: The economic burden associated with type 2 diabetes mellitus (T2DM) and concurrent cardiovascular disease (CVD) among patients with COVID-19 is unclear. Objective: We compared healthcare resource utilization (HCRU) and costs in patients with COVID-19 and T2DM and CVD (T2DM + CVD), T2DM only, or neither T2DM nor CVD (T2DM/CVD). Methods: A retrospective observational study in COVID-19 patients using data from the Healthcare Integrated Research Database (HIRD®) was conducted. Patients with COVID-19 were identified between March 1, 2020, and May 31, 2021, and followed from first diagnosis or positive lab test to the end of health plan enrollment, end of study period, or death. Patients were assigned one of 3 cohorts: pre-existing T2DM+CVD, T2DM only, or neither T2DM/CVD. Propensity score matching and multivariable analyses were performed to control for differences in baseline characteristics. Study outcomes included all-cause and COVID-19-related HCRU and costs. Results: In all, 321 232 COVID-19 patients were identified (21 651 with T2DM + CVD, 28 184 with T2DM only, and 271 397 with neither T2DM/CVD). After matching, 6967 patients were in each group. Before matching, 46.0% of patients in the T2DM + CVD cohort were hospitalized for any cause, compared with 18.0% in the T2DM-only cohort and 6.3% in the neither T2DM/CVD cohort; the corresponding values after matching were 34.2%, 26.0%, and 21.2%. The proportion of patients with emergency department visits, telehealth visits, or use of skilled nursing facilities was higher in patients with COVID-19 and T2DM + CVD compared with the other cohorts. Average all-cause costs during follow-up were 7882, and $7277 per-patient-per-month after matching for patients with T2DM + CVD, T2DM-only, and neither T2DM/CVD, respectively. COVID-19-related costs contributed to 78%, 75%, and 64% of the overall costs, respectively. The multivariable model showed that per-patient-per-month all-cause costs for T2DM + CVD and T2DM-only were 54% and 21% higher, respectively, than those with neither T2DM/CVD after adjusting for residual confounding. Conclusion: HCRU and costs in patients were incrementally higher with COVID-19 and pre-existing T2DM + CVD compared with those with T2DM-only and neither T2DM/CVD, even after accounting for baseline differences between groups, confirming that pre-existing T2DM + CVD is associated with increased HCRU and costs in COVID-19 patients, highlighting the importance of proactive management.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
