Yajuan Gao, Shengnan Chen, Jiani Fu, Cui Wang, Yali Tang, Yongbai Luo, Xiaozhen Zhuo, Xueying Chen, Yan Shen
{"title":"Factors associated with risk analysis for asymptomatic left ventricular diastolic dysfunction in nondialysis patients with chronic kidney disease.","authors":"Yajuan Gao, Shengnan Chen, Jiani Fu, Cui Wang, Yali Tang, Yongbai Luo, Xiaozhen Zhuo, Xueying Chen, Yan Shen","doi":"10.1080/0886022X.2024.2353334","DOIUrl":null,"url":null,"abstract":"<p><p>Heart failure (HF) constitutes a major determinant of outcome in chronic kidney disease (CKD) patients. The main pattern of HF in CKD patients is preserved ejection fraction (HFpEF), and left ventricular diastolic dysfunction (LVDD) is a frequent pathophysiological mechanism and specific preclinical manifestation of HFpEF. Therefore, exploring and intervention of the factors associated with risk for LVDD is of great importance in reducing the morbidity and mortality of cardiovascular disease (CVD) complications in CKD patients. We designed this retrospective cross-sectional study to collect clinical and echocardiographic data from 339 nondialysis CKD patients without obvious symptoms of HF to analyze the proportion of asymptomatic left ventricular diastolic dysfunction (ALVDD) and its related factors associated with risk by multivariate logistic regression analysis. Among the 339 nondialysis CKD patients, 92.04% had ALVDD. With the progression of CKD stage, the proportion of ALVDD gradually increased. The multivariate logistic regression analysis revealed that increased age (OR 1.237; 95% confidence interval (CI) 1.108-1.381, per year), diabetic nephropathy (DN) and hypertensive nephropathy (HTN) (OR 25.000; 95% CI 1.355-48.645, DN and HTN <i>vs</i> chronic interstitial nephritis), progression of CKD stage (OR 2.785; 95% CI 1.228-6.315, per stage), increased mean arterial pressure (OR 1.154; 95% CI 1.051-1.268, per mmHg), increased urinary protein (OR 2.825; 95% CI 1.484-5.405, per g/24 h), and low blood calcium (OR 0.072; 95% CI 0.006-0.859, per mmol/L) were factors associated with risk for ALVDD in nondialysis CKD patients after adjusting for other confounding factors. Therefore, dynamic monitoring of these factors associated with risk, timely diagnosis and treatment of ALVDD can delay the progression to symptomatic HF, which is of great importance for reducing CVD mortality, and improving the prognosis and quality of life in CKD patients.</p>","PeriodicalId":20839,"journal":{"name":"Renal Failure","volume":"46 1","pages":"2353334"},"PeriodicalIF":3.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11133225/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Renal Failure","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/0886022X.2024.2353334","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/24 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
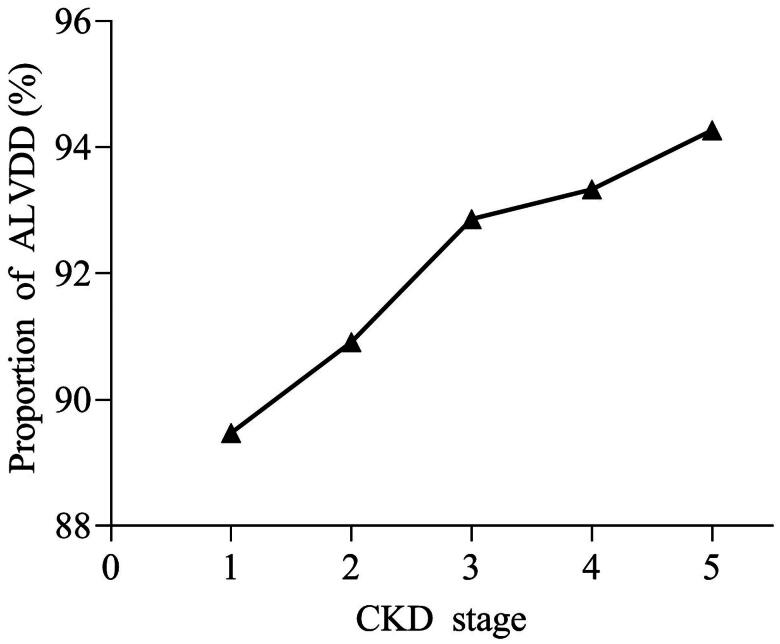
Heart failure (HF) constitutes a major determinant of outcome in chronic kidney disease (CKD) patients. The main pattern of HF in CKD patients is preserved ejection fraction (HFpEF), and left ventricular diastolic dysfunction (LVDD) is a frequent pathophysiological mechanism and specific preclinical manifestation of HFpEF. Therefore, exploring and intervention of the factors associated with risk for LVDD is of great importance in reducing the morbidity and mortality of cardiovascular disease (CVD) complications in CKD patients. We designed this retrospective cross-sectional study to collect clinical and echocardiographic data from 339 nondialysis CKD patients without obvious symptoms of HF to analyze the proportion of asymptomatic left ventricular diastolic dysfunction (ALVDD) and its related factors associated with risk by multivariate logistic regression analysis. Among the 339 nondialysis CKD patients, 92.04% had ALVDD. With the progression of CKD stage, the proportion of ALVDD gradually increased. The multivariate logistic regression analysis revealed that increased age (OR 1.237; 95% confidence interval (CI) 1.108-1.381, per year), diabetic nephropathy (DN) and hypertensive nephropathy (HTN) (OR 25.000; 95% CI 1.355-48.645, DN and HTN vs chronic interstitial nephritis), progression of CKD stage (OR 2.785; 95% CI 1.228-6.315, per stage), increased mean arterial pressure (OR 1.154; 95% CI 1.051-1.268, per mmHg), increased urinary protein (OR 2.825; 95% CI 1.484-5.405, per g/24 h), and low blood calcium (OR 0.072; 95% CI 0.006-0.859, per mmol/L) were factors associated with risk for ALVDD in nondialysis CKD patients after adjusting for other confounding factors. Therefore, dynamic monitoring of these factors associated with risk, timely diagnosis and treatment of ALVDD can delay the progression to symptomatic HF, which is of great importance for reducing CVD mortality, and improving the prognosis and quality of life in CKD patients.
期刊介绍:
Renal Failure primarily concentrates on acute renal injury and its consequence, but also addresses advances in the fields of chronic renal failure, hypertension, and renal transplantation. Bringing together both clinical and experimental aspects of renal failure, this publication presents timely, practical information on pathology and pathophysiology of acute renal failure; nephrotoxicity of drugs and other substances; prevention, treatment, and therapy of renal failure; renal failure in association with transplantation, hypertension, and diabetes mellitus.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
