Extremely long RNS implantation effect: The extended impact of RNS electrodes on clinical and ECoG findings without the confounding effect of RNS stimulation
Matthew T. Rumschlag, Kalina A. Misiolek, Prachi Parikh, Ifrah Zawar
{"title":"Extremely long RNS implantation effect: The extended impact of RNS electrodes on clinical and ECoG findings without the confounding effect of RNS stimulation","authors":"Matthew T. Rumschlag, Kalina A. Misiolek, Prachi Parikh, Ifrah Zawar","doi":"10.1002/epd2.20233","DOIUrl":null,"url":null,"abstract":"<p>Implantation effect is the phenomenon of a transient decrease in clinical seizure frequency following the placement of intracranial electrodes or neuromodulatory devices.<span><sup>1</sup></span> This effect has been demonstrated in different procedures such as stereo-EEG, deep brain stimulation, and subdural strips or grids.<span><sup>2-4</sup></span> This effect is typically thought to last for no longer than a few months.<span><sup>5, 6</sup></span> Recently, Responsive Neurostimulation (RNS) system (NeuroPace, Inc.) electrode placement has also demonstrated similar transient improvement in clinical seizure frequency.<span><sup>3</sup></span> Electrocorticographic (ECoG) spectral power changes and reduction in spike rates have also been described for up to 5 months of chronic ECoG in RNS patients.<span><sup>7</sup></span> However, RNS stimulation is routinely turned on within a few weeks of implantation.<span><sup>3, 7</sup></span> Therefore, the degree to which RNS implantation versus stimulation leads to long-term clinical and electrophysiologic changes beyond the initial post-implant period is unclear.</p><p>To our knowledge, no previous studies have investigated the impact of RNS implantation on long episodes and electrographic seizures in patients not receiving RNS stimulation. Long episodes refer to any pattern that meets the RNS detection threshold but without evolution, whereas electrographic seizures constitute a pattern with distinct evolution. Here, we describe a patient who underwent bilateral RNS implantation and remained free of clinical seizures for at least 2 years and 1 month and free of long episodes and electrographic seizures for 14 months with no RNS stimulation during the initial 8-month period. Informed consent was obtained.</p><p>A 19-year-old woman with a longstanding history of drug-resistant focal epilepsy with focal seizures with impaired awareness, with and without secondary generalization underwent presurgical evaluation. At baseline, she had five to nine seizures per month. The longest seizure-free period prior to RNS was a few months. Stereo-EEG confirmed independent seizures arising from (Figure 1) bilateral hippocampi (Table 1). She underwent RNS implantation with bilateral hippocampal leads, after which she remained seizure-free. Given her lack of clinical and electrographic seizures, long episodes, or other epileptiform activity on ECoG, RNS stimulation was not turned on for 8 months post-implantation. At 8 months, RNS stimulation was ultimately turned on at the suggestion of the NeuroPace team despite the continued lack of clinical or electrographic events. After self-weaning anti-seizure medications (ASMs), she started to have rare long episodes and electrographic seizures at 14 months. These resolved after increasing her ASMs back to their original doses. She continues to remain completely free of clinical seizures at 2 years and 1 month post-implantation.</p><p>Our case demonstrates the extended impact of RNS electrodes on clinical and ECoG findings without the confounding effect of RNS stimulation. Most often, cases of implantation effect following RNS placement report on clinical seizure freedom but do not comment on the presence or absence of ECoG changes.<span><sup>3</sup></span> RNS stimulation is usually turned on within weeks to months of implantation. Thus, it remains unclear whether seizure freedom is truly due to the implantation itself or due to the stimulation.<span><sup>3, 8, 9</sup></span> The lack of RNS stimulation for the initial 8-month period in our patient eliminates the usual confounding effect of stimulation and suggests that the lack of ECoG changes, long episodes, and electrographic seizures was most likely due to the electrodes alone.</p><p>In terms of clinical seizures, to date, our patient continues to remain free of clinical seizures at 2 years. There are rare reports of implantation effect resulting in seizure freedom for many months to years in patients undergoing intracranial monitoring.<span><sup>10-13</sup></span> To our knowledge, this has not been described in the literature following RNS implantation.</p><p>Although its pathophysiology is not known, it has been hypothesized that the insertion of intracranial electrodes may create microlesions that disrupt epileptic networks.<span><sup>4, 10-12</sup></span> Some cases of implantation effect describe obvious MRI changes or edema suggesting a lesional effect,<span><sup>11</sup></span> while others describe unchanged or minimally changed post-implantation MRIs.<span><sup>4, 10</sup></span> Other hypotheses include perioperative medications or anesthesia or persistent neuroinflammation due to the presence of the electrode.<span><sup>4, 12</sup></span></p><p>Our case suggests that although the standard practice is to turn on RNS stimulation shortly following implantation, perhaps the decision about when and whether or not to start stimulation should be based on clinical and ECoG findings specific to each patient. Furthermore, while the current standard of practice with resective surgery or laser ablation is to target the entire epileptogenic zone, our case suggests that creating microlesions could be explored as an alternative treatment in future trials, especially in regions close to the eloquent cortex.</p><p>In conclusion, our findings add to the growing evidence that placement of RNS leads has the potential to result not just in long-term clinical seizure freedom but also in long-lasting electrographic changes.</p><p>This research work did not receive funding. Dr Zawar receives funding from Alzheimer's Association and American Epilepsy Society. None of the other authors have any other funding to declare.</p><p>None of the authors have any conflict of interests to disclose.</p>","PeriodicalId":50508,"journal":{"name":"Epileptic Disorders","volume":"26 4","pages":"536-539"},"PeriodicalIF":2.7000,"publicationDate":"2024-05-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/epd2.20233","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epileptic Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/epd2.20233","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Implantation effect is the phenomenon of a transient decrease in clinical seizure frequency following the placement of intracranial electrodes or neuromodulatory devices.1 This effect has been demonstrated in different procedures such as stereo-EEG, deep brain stimulation, and subdural strips or grids.2-4 This effect is typically thought to last for no longer than a few months.5, 6 Recently, Responsive Neurostimulation (RNS) system (NeuroPace, Inc.) electrode placement has also demonstrated similar transient improvement in clinical seizure frequency.3 Electrocorticographic (ECoG) spectral power changes and reduction in spike rates have also been described for up to 5 months of chronic ECoG in RNS patients.7 However, RNS stimulation is routinely turned on within a few weeks of implantation.3, 7 Therefore, the degree to which RNS implantation versus stimulation leads to long-term clinical and electrophysiologic changes beyond the initial post-implant period is unclear.
To our knowledge, no previous studies have investigated the impact of RNS implantation on long episodes and electrographic seizures in patients not receiving RNS stimulation. Long episodes refer to any pattern that meets the RNS detection threshold but without evolution, whereas electrographic seizures constitute a pattern with distinct evolution. Here, we describe a patient who underwent bilateral RNS implantation and remained free of clinical seizures for at least 2 years and 1 month and free of long episodes and electrographic seizures for 14 months with no RNS stimulation during the initial 8-month period. Informed consent was obtained.
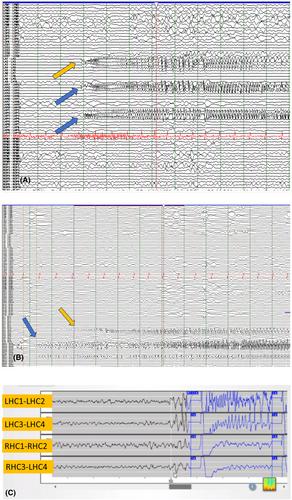
A 19-year-old woman with a longstanding history of drug-resistant focal epilepsy with focal seizures with impaired awareness, with and without secondary generalization underwent presurgical evaluation. At baseline, she had five to nine seizures per month. The longest seizure-free period prior to RNS was a few months. Stereo-EEG confirmed independent seizures arising from (Figure 1) bilateral hippocampi (Table 1). She underwent RNS implantation with bilateral hippocampal leads, after which she remained seizure-free. Given her lack of clinical and electrographic seizures, long episodes, or other epileptiform activity on ECoG, RNS stimulation was not turned on for 8 months post-implantation. At 8 months, RNS stimulation was ultimately turned on at the suggestion of the NeuroPace team despite the continued lack of clinical or electrographic events. After self-weaning anti-seizure medications (ASMs), she started to have rare long episodes and electrographic seizures at 14 months. These resolved after increasing her ASMs back to their original doses. She continues to remain completely free of clinical seizures at 2 years and 1 month post-implantation.
Our case demonstrates the extended impact of RNS electrodes on clinical and ECoG findings without the confounding effect of RNS stimulation. Most often, cases of implantation effect following RNS placement report on clinical seizure freedom but do not comment on the presence or absence of ECoG changes.3 RNS stimulation is usually turned on within weeks to months of implantation. Thus, it remains unclear whether seizure freedom is truly due to the implantation itself or due to the stimulation.3, 8, 9 The lack of RNS stimulation for the initial 8-month period in our patient eliminates the usual confounding effect of stimulation and suggests that the lack of ECoG changes, long episodes, and electrographic seizures was most likely due to the electrodes alone.
In terms of clinical seizures, to date, our patient continues to remain free of clinical seizures at 2 years. There are rare reports of implantation effect resulting in seizure freedom for many months to years in patients undergoing intracranial monitoring.10-13 To our knowledge, this has not been described in the literature following RNS implantation.
Although its pathophysiology is not known, it has been hypothesized that the insertion of intracranial electrodes may create microlesions that disrupt epileptic networks.4, 10-12 Some cases of implantation effect describe obvious MRI changes or edema suggesting a lesional effect,11 while others describe unchanged or minimally changed post-implantation MRIs.4, 10 Other hypotheses include perioperative medications or anesthesia or persistent neuroinflammation due to the presence of the electrode.4, 12
Our case suggests that although the standard practice is to turn on RNS stimulation shortly following implantation, perhaps the decision about when and whether or not to start stimulation should be based on clinical and ECoG findings specific to each patient. Furthermore, while the current standard of practice with resective surgery or laser ablation is to target the entire epileptogenic zone, our case suggests that creating microlesions could be explored as an alternative treatment in future trials, especially in regions close to the eloquent cortex.
In conclusion, our findings add to the growing evidence that placement of RNS leads has the potential to result not just in long-term clinical seizure freedom but also in long-lasting electrographic changes.
This research work did not receive funding. Dr Zawar receives funding from Alzheimer's Association and American Epilepsy Society. None of the other authors have any other funding to declare.
None of the authors have any conflict of interests to disclose.
期刊介绍:
Epileptic Disorders is the leading forum where all experts and medical studentswho wish to improve their understanding of epilepsy and related disorders can share practical experiences surrounding diagnosis and care, natural history, and management of seizures.
Epileptic Disorders is the official E-journal of the International League Against Epilepsy for educational communication. As the journal celebrates its 20th anniversary, it will now be available only as an online version. Its mission is to create educational links between epileptologists and other health professionals in clinical practice and scientists or physicians in research-based institutions. This change is accompanied by an increase in the number of issues per year, from 4 to 6, to ensure regular diffusion of recently published material (high quality Review and Seminar in Epileptology papers; Original Research articles or Case reports of educational value; MultiMedia Teaching Material), to serve the global medical community that cares for those affected by epilepsy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
