Peter Calvert MBChB, Yang Chen MBChB, Ying Gue PhD, Dhiraj Gupta MD, Jinbert Lordson Azariah MSc, A. George Koshy MD, Geevar Zachariah MD, Gregory Y. H. Lip MD, Bahuleyan Charantharayil Gopalan MD, the Kerala AF Registry Investigators
{"title":"One-year outcomes of rate versus rhythm control of atrial fibrillation in the Kerala-AF Registry","authors":"Peter Calvert MBChB, Yang Chen MBChB, Ying Gue PhD, Dhiraj Gupta MD, Jinbert Lordson Azariah MSc, A. George Koshy MD, Geevar Zachariah MD, Gregory Y. H. Lip MD, Bahuleyan Charantharayil Gopalan MD, the Kerala AF Registry Investigators","doi":"10.1002/joa3.13059","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>There is ongoing debate around rate versus rhythm control strategies for managing atrial fibrillation (AF), however, much of the data comes from Western cohorts. Kerala-AF represents the largest prospective AF cohort study from the Indian subcontinent.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>To compare 12-month outcomes between rate and rhythm control strategies.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients aged ≥18 years with non-transient AF were recruited from 53 hospitals across Kerala. Patients were stratified by rate or rhythm control. The primary outcome was a composite of all-cause mortality, arterial thromboembolism, acute coronary syndrome or hospitalization due to heart failure or arrhythmia at 12 months. Secondary outcomes included bleeding events and individual components of the primary. Predictors of the composite outcome were analysed by logistic regression.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 2901 patients (mean age 64.6 years, 51% female) were included (2464 rate control, 437 rhythm control). Rates of the primary composite outcome did not differ between groups (29.7% vs 30.0%; <i>p</i> = .955), nor did any component of the primary. Bleeding outcomes were also similar (1.6% vs 1.9%; <i>p</i> = .848). Independent predictors of the primary composite outcome were older age (aOR 1.01; <i>p</i> = .013), BMI <18 (aOR 1.51; <i>p</i> = .025), permanent AF (aOR 0.78; <i>p</i> = .010), HFpEF (aOR 1.40; <i>p</i> = .023), HFrEF (aOR 1.39; <i>p</i> = .004), chronic kidney disease (aOR 1.36; <i>p</i> < .001), and prior thromboembolism (aOR 1.31; <i>p</i> = .014).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In the Kerala-AF registry, 12-month outcomes did not differ between rate and rhythm control cohorts.</p>\n </section>\n </div>","PeriodicalId":15174,"journal":{"name":"Journal of Arrhythmia","volume":"40 4","pages":"822-829"},"PeriodicalIF":1.7000,"publicationDate":"2024-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/joa3.13059","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Arrhythmia","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/joa3.13059","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
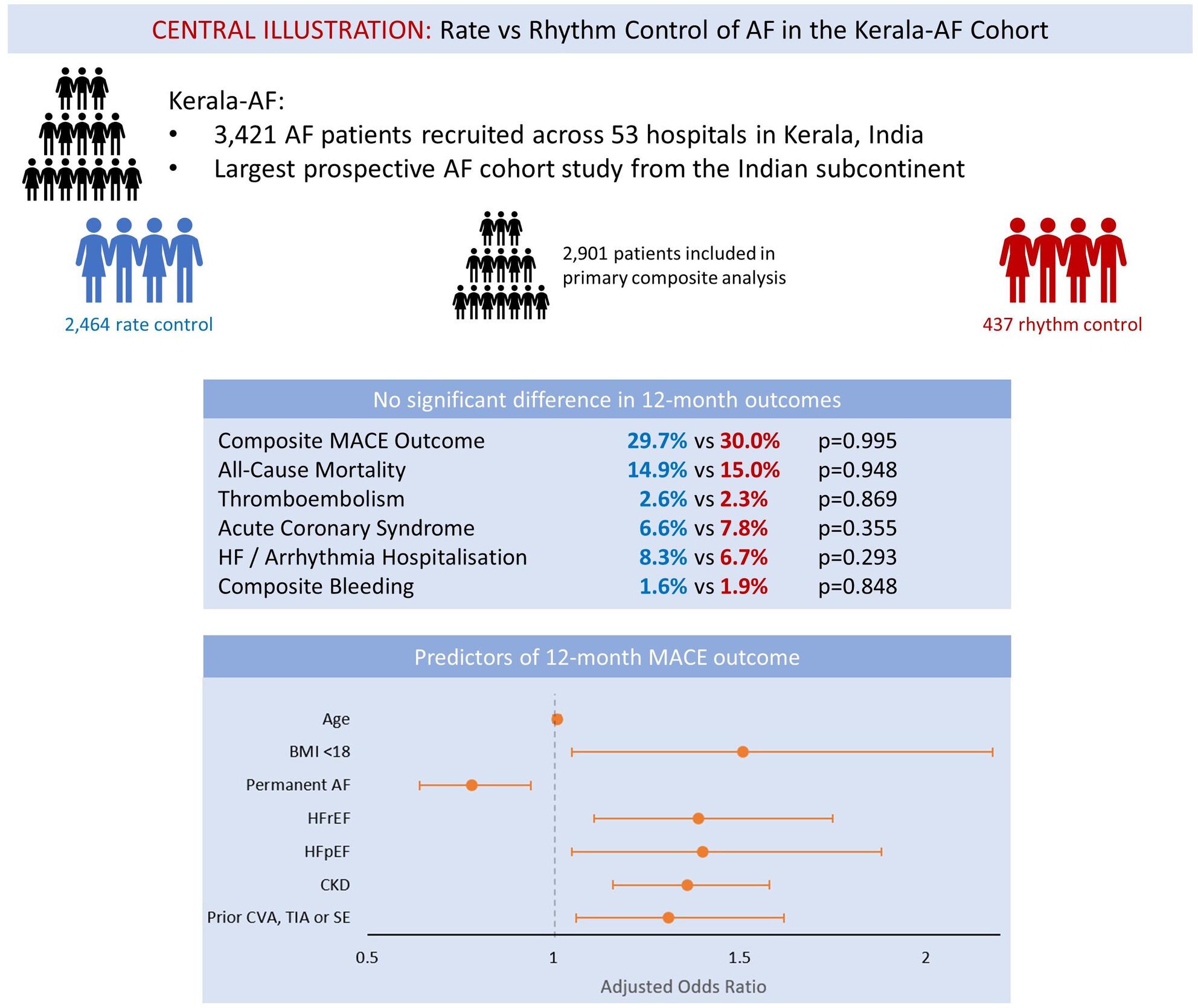
There is ongoing debate around rate versus rhythm control strategies for managing atrial fibrillation (AF), however, much of the data comes from Western cohorts. Kerala-AF represents the largest prospective AF cohort study from the Indian subcontinent.
Objectives
To compare 12-month outcomes between rate and rhythm control strategies.
Methods
Patients aged ≥18 years with non-transient AF were recruited from 53 hospitals across Kerala. Patients were stratified by rate or rhythm control. The primary outcome was a composite of all-cause mortality, arterial thromboembolism, acute coronary syndrome or hospitalization due to heart failure or arrhythmia at 12 months. Secondary outcomes included bleeding events and individual components of the primary. Predictors of the composite outcome were analysed by logistic regression.
Results
A total of 2901 patients (mean age 64.6 years, 51% female) were included (2464 rate control, 437 rhythm control). Rates of the primary composite outcome did not differ between groups (29.7% vs 30.0%; p = .955), nor did any component of the primary. Bleeding outcomes were also similar (1.6% vs 1.9%; p = .848). Independent predictors of the primary composite outcome were older age (aOR 1.01; p = .013), BMI <18 (aOR 1.51; p = .025), permanent AF (aOR 0.78; p = .010), HFpEF (aOR 1.40; p = .023), HFrEF (aOR 1.39; p = .004), chronic kidney disease (aOR 1.36; p < .001), and prior thromboembolism (aOR 1.31; p = .014).
Conclusion
In the Kerala-AF registry, 12-month outcomes did not differ between rate and rhythm control cohorts.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
