{"title":"An unusual presentation of ischemic bowel disease","authors":"Chien-Tzu Hung, Chien-Chih Tung","doi":"10.1002/aid2.13403","DOIUrl":null,"url":null,"abstract":"<p>A 60-year-old previously healthy woman presented with a sudden onset of lower abdominal pain followed by watery diarrhea after hiking. A CT scan revealed portal venous gas (Figure 1A) and heterogeneous hypoattenuating wall thickening over the terminal ileum, without other lesions in the major vessels (Figure 1B). She left against medical advice but returned later with worsened abdominal pain and hematochezia. On examination, tachycardia (103 beats per minute), tachypnea (22 breaths per minute), and tenderness over the lower abdomen were recorded. Laboratory investigation revealed leukocytosis (1645/mL), azotemia (blood urea nitrogen is 29.3 mg/dL), lactic acidosis (2.75 mmol/L), and hyperglycemia (322 mg/dL). A colonoscopy revealed shallow ulcers with exudative discharge from 4 to 10 cm above the ileocecal valve (Figure 2). Biopsy showed ulcer debris, hyalinization of the lamina propria, smaller and decreased number of glands, which were compatible with ischemic change. Stool culture, tissue culture, and autoimmune profile were all negative. A diagnosis of ischemic ileitis was made, and the symptoms resolved under supportive care and empirical flomoxef. She was also diagnosed of type 2 diabetes mellitus and treatment was then started. Following colonoscopy 6 months later showed normal mucosa.</p><p>Ischemic bowel disease could be divided into colonic and mesenteric ischemia. Colonic ischemia is the most common form and has a more favorable outcome.<span><sup>1</sup></span> The possible etiology of this event could be dehydration due to hiking and a hyperglycemic state. The isolated ischemic change of the terminal ileum is unusual, since it is not in the traditional watershed zones.<span><sup>2</sup></span> Ileitis may result from a variety of disease such as Crohn's disease, infection, spondyloarthropathies, vasculitides, ischemia, neoplasms, medication-induced, and eosinophilic enteritis.<span><sup>3</sup></span></p><p>We presented a case of ischemic ileitis, highlighting the importance of a comprehensive diagnostic approach and consideration of various etiologies.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 3","pages":"177-178"},"PeriodicalIF":0.4000,"publicationDate":"2024-05-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13403","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13403","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
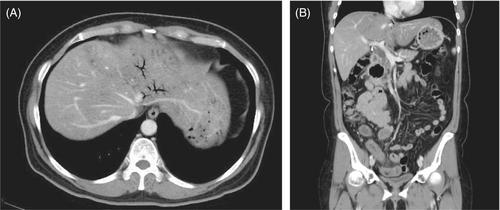
A 60-year-old previously healthy woman presented with a sudden onset of lower abdominal pain followed by watery diarrhea after hiking. A CT scan revealed portal venous gas (Figure 1A) and heterogeneous hypoattenuating wall thickening over the terminal ileum, without other lesions in the major vessels (Figure 1B). She left against medical advice but returned later with worsened abdominal pain and hematochezia. On examination, tachycardia (103 beats per minute), tachypnea (22 breaths per minute), and tenderness over the lower abdomen were recorded. Laboratory investigation revealed leukocytosis (1645/mL), azotemia (blood urea nitrogen is 29.3 mg/dL), lactic acidosis (2.75 mmol/L), and hyperglycemia (322 mg/dL). A colonoscopy revealed shallow ulcers with exudative discharge from 4 to 10 cm above the ileocecal valve (Figure 2). Biopsy showed ulcer debris, hyalinization of the lamina propria, smaller and decreased number of glands, which were compatible with ischemic change. Stool culture, tissue culture, and autoimmune profile were all negative. A diagnosis of ischemic ileitis was made, and the symptoms resolved under supportive care and empirical flomoxef. She was also diagnosed of type 2 diabetes mellitus and treatment was then started. Following colonoscopy 6 months later showed normal mucosa.
Ischemic bowel disease could be divided into colonic and mesenteric ischemia. Colonic ischemia is the most common form and has a more favorable outcome.1 The possible etiology of this event could be dehydration due to hiking and a hyperglycemic state. The isolated ischemic change of the terminal ileum is unusual, since it is not in the traditional watershed zones.2 Ileitis may result from a variety of disease such as Crohn's disease, infection, spondyloarthropathies, vasculitides, ischemia, neoplasms, medication-induced, and eosinophilic enteritis.3
We presented a case of ischemic ileitis, highlighting the importance of a comprehensive diagnostic approach and consideration of various etiologies.
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
