Several protective factors have been identified for mental health (MH) resilience in adolescent offspring of depressed parents. However, it is unclear if these effects persist into adulthood.
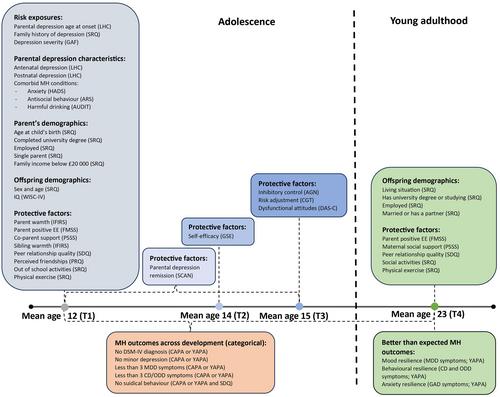
Depressed parents and their offspring (N = 188) from the Early Prediction of Adolescent Depression study were assessed four times (mean offspring ages 12.39, 13.77, 14.82, and 23.41). Mental health resilience was examined using residual scores (better-than-expected mood-, behaviour-, or anxiety-related MH at mean age 23 given risk exposure), and categorically as sustained good MH across adolescence and young adulthood.
Only 9.2% of young adults demonstrated sustained good MH. Parents of resilient individuals showed lower comorbidity (anxiety, antisocial behaviour and harmful drinking) and higher depression remission. Considering adolescent protective factors, weak evidence was observed of associations of mood-resilience with adolescent peer-relationship quality (β = −0.20, 95%CI:−0.36, −0.04); friendship quality (β = −0.14, 95%CI:−0.31, 0.02); risk adjustment (β = −0.16, 95%CI:-0.34, 0.03) and dysfunctional attitudes (β = 0.18, 95%CI:0.01, 0.35). There was weak evidence of behavioural-resilience association with parent positive expressed emotion (β = −0.15, 95%CI:−0.31, 0.02) and offspring exercise (β = −0.37, 95%CI:−0.77, 0.03). No adolescent protective factors showed an association with anxiety-resilience. For sustained good MH, there was weak evidence of an association with inhibitory control (OR = 0.39, 95%CI:0.14, 1.07). Strong evidence was observed for associations between young adult-reported peer relationship quality and mood-resilience (β = −0.35, 95%CI:−0.53, −0.17), behavioural-resilience (β = −0.33, 95%CI:−0.51, −0.14) and anxiety-resilience (β = −0.34, 95%CI:−0.53, −0.14), while weak evidence was observed of an association of social activities with anxiety-resilience (β = −0.51, 95%CI:−0.97, −0.06).
We found limited evidence for the long-lasting effects of adolescent protective factors on adult MH resilience. Social factors remained protective into young adulthood, while family factors did not. Early preventative intervention might not be sufficient to maintain good long-term MH, and young people will likely require more prolonged support.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
