Amanda Corley RN, MAdvPrac, PhD, Ruth H. Royle RN, MEcon, Nicole Marsh RN, MAdvPrac, PhD, Emily N. Larsen RN, GDipHlthRes, PhD (Cand), E. Geoffrey Playford MBBS (Hons), MMed (Clin Epi), PhD, FRACP, FRCPA, Matthew R. McGrail PhD, Naomi Runnegar MBBS, FRACP, FRCPA, Robert S. Ware BSc, PhD, Nicole C. Gavin RN, MAdvPrac, PhD, Evan Alexandrou RN, PhD, Marghie Murgo RN, MCritCareNurs, John R. Gowardman MBChB, FCICM, FRACP, Adrian Regli MD, PhD, FCICM, Claire M. Rickard RN, PhD
{"title":"Incidence and risk factors for central venous access device failure in hospitalized adults: A multivariable analysis of 1892 catheters","authors":"Amanda Corley RN, MAdvPrac, PhD, Ruth H. Royle RN, MEcon, Nicole Marsh RN, MAdvPrac, PhD, Emily N. Larsen RN, GDipHlthRes, PhD (Cand), E. Geoffrey Playford MBBS (Hons), MMed (Clin Epi), PhD, FRACP, FRCPA, Matthew R. McGrail PhD, Naomi Runnegar MBBS, FRACP, FRCPA, Robert S. Ware BSc, PhD, Nicole C. Gavin RN, MAdvPrac, PhD, Evan Alexandrou RN, PhD, Marghie Murgo RN, MCritCareNurs, John R. Gowardman MBChB, FCICM, FRACP, Adrian Regli MD, PhD, FCICM, Claire M. Rickard RN, PhD","doi":"10.1002/jhm.13414","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Central venous access devices (CVADs) allow intravenous therapy, haemodynamic monitoring and blood sampling but many fail before therapy completion.</p>\n </section>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>To quantify CVAD failure and complications; and identify risk factors.</p>\n </section>\n \n <section>\n \n <h3> Designs, Settings, and Participants</h3>\n \n <p>Secondary analysis of multicentre randomised controlled trial including patients aged ≥16 years with a non-tunnelled CVAD (NTCVAD), peripherally-inserted central catheter (PICC) or tunnelled CVAD (TCVAD). Primary outcome was incidence of all-cause CVAD failure (central line-associated bloodstream infection [CLABSI], occlusion, accidental dislodgement, catheter fracture, thrombosis, pain). Secondary outcomes were CLABSI, occlusion and dislodgement. Cox regression was used to report time-to-event associations.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In 1892 CVADs, all-cause failure occurred in 10.2% of devices: 49 NTCVADs (6.1%); 100 PICCs (13.2%); 44 TCVADs (13.4%). Failure rates for CLABSI, occlusion and dislodgement were 5.3%, 1.8%, and 1.7%, respectively. Independent CLABSI predictors were blood product administration through PICCs (hazard ratio (HR) 2.62, 95% confidence interval (CI) 1.24–5.55); and in TCVADs, one or two lumens, compared with three to four (HR 3.36, 95%CI 1.68–6.71), intravenous chemotherapy (HR 2.96, 95%CI 1.31–6.68), and diabetes (HR 3.25, 95%CI 1.40–7.57). Independent factors protective for CLABSI include antimicrobial NTCVADs (HR 0.23, 95%CI 0.08–0.63) and lipids in TCVADs (HR 0.32, 95%CI 0.14–0.72). NTCVADs inserted at another hospital (HR 7.06, 95%CI 1.48–33.7) and baseline infection in patients with PICCs (HR 2.72, 95%CI 1.08–6.83) were predictors for dislodgement. No independent occlusion predictors were found. Modifiable risk factors were identified for CVAD failure, which occurred for 1-in-10 catheters. Strict infection prevention measures and improved CVAD securement could reduce CLABSI and dislodgement risk.</p>\n </section>\n </div>","PeriodicalId":15883,"journal":{"name":"Journal of hospital medicine","volume":"19 10","pages":"905-917"},"PeriodicalIF":2.3000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhm.13414","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hospital medicine","FirstCategoryId":"3","ListUrlMain":"https://shmpublications.onlinelibrary.wiley.com/doi/10.1002/jhm.13414","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Central venous access devices (CVADs) allow intravenous therapy, haemodynamic monitoring and blood sampling but many fail before therapy completion.
Objective
To quantify CVAD failure and complications; and identify risk factors.
Designs, Settings, and Participants
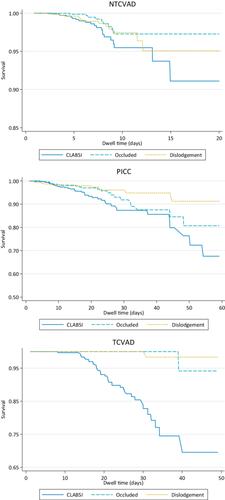
Secondary analysis of multicentre randomised controlled trial including patients aged ≥16 years with a non-tunnelled CVAD (NTCVAD), peripherally-inserted central catheter (PICC) or tunnelled CVAD (TCVAD). Primary outcome was incidence of all-cause CVAD failure (central line-associated bloodstream infection [CLABSI], occlusion, accidental dislodgement, catheter fracture, thrombosis, pain). Secondary outcomes were CLABSI, occlusion and dislodgement. Cox regression was used to report time-to-event associations.
Results
In 1892 CVADs, all-cause failure occurred in 10.2% of devices: 49 NTCVADs (6.1%); 100 PICCs (13.2%); 44 TCVADs (13.4%). Failure rates for CLABSI, occlusion and dislodgement were 5.3%, 1.8%, and 1.7%, respectively. Independent CLABSI predictors were blood product administration through PICCs (hazard ratio (HR) 2.62, 95% confidence interval (CI) 1.24–5.55); and in TCVADs, one or two lumens, compared with three to four (HR 3.36, 95%CI 1.68–6.71), intravenous chemotherapy (HR 2.96, 95%CI 1.31–6.68), and diabetes (HR 3.25, 95%CI 1.40–7.57). Independent factors protective for CLABSI include antimicrobial NTCVADs (HR 0.23, 95%CI 0.08–0.63) and lipids in TCVADs (HR 0.32, 95%CI 0.14–0.72). NTCVADs inserted at another hospital (HR 7.06, 95%CI 1.48–33.7) and baseline infection in patients with PICCs (HR 2.72, 95%CI 1.08–6.83) were predictors for dislodgement. No independent occlusion predictors were found. Modifiable risk factors were identified for CVAD failure, which occurred for 1-in-10 catheters. Strict infection prevention measures and improved CVAD securement could reduce CLABSI and dislodgement risk.
期刊介绍:
JHM is a peer-reviewed publication of the Society of Hospital Medicine and is published 12 times per year. JHM publishes manuscripts that address the care of hospitalized adults or children.
Broad areas of interest include (1) Treatments for common inpatient conditions; (2) Approaches to improving perioperative care; (3) Improving care for hospitalized patients with geriatric or pediatric vulnerabilities (such as mobility problems, or those with complex longitudinal care); (4) Evaluation of innovative healthcare delivery or educational models; (5) Approaches to improving the quality, safety, and value of healthcare across the acute- and postacute-continuum of care; and (6) Evaluation of policy and payment changes that affect hospital and postacute care.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
