Catherine C Allen, Briana L Swanson, Xiao Zhang, Ryan J Coller, Krisjon R Olson
{"title":"Quality Improvement Identifies Healthcare Transition Disparities in Adolescents with Congenital Heart Disease and Disabilities.","authors":"Catherine C Allen, Briana L Swanson, Xiao Zhang, Ryan J Coller, Krisjon R Olson","doi":"10.1097/pq9.0000000000000732","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>We aim to implement healthcare transition (HCT) education for youth with congenital heart disease (CHD) and assess HCT preparedness for cardiac self-care.</p><p><strong>Methods: </strong>An HCT clinic was implemented at an academic pediatric cardiology clinic for CHD youth 17 years of age and older. An educator used transition readiness assessment questionnaires and discussed HCT material. The percentage of eligible youth who received HCT education and the cause for missed occurrences were tracked. Plan-do-study-act cycles began in August 2020 to improve the number of youths reached. Secondary analyses assessed improvement differences among those without cardiac procedures or disabilities.</p><p><strong>Results: </strong>HCT education provision improved from a mean of 38% to 73% in the 17-year and older age group by December 2022. Communication failure was the leading cause of missed visits in 2021 (30%), reduced to 0 by 2022 following plan-do-study-act cycles. Other missed HCT visits included clinic add-ons after screening, limited staff availability, and unidentified eligibility. Readiness assessments were similar for youth with and without prior cardiac procedures, for example, confidence in taking charge of their health care (<i>P</i> = 0.47) and moving to adult care (<i>P</i> = 0.22). Adolescents with disabilities were significantly less confident than those without disabilities in taking charge of their heart health care (6.3 versus 7.5, <i>P</i> = 0.04) and moving to adult care (4.9 versus 7.4, <i>P</i> < 0.001).</p><p><strong>Conclusions: </strong>Implementation of a CHD HCT clinic improved successful education delivery. Provider engagement and clinic staffing are important for sustainability. HCT knowledge gaps exist for all adolescents, yet those with disabilities had the greatest deficits.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 3","pages":"e732"},"PeriodicalIF":1.1000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11132416/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000732","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
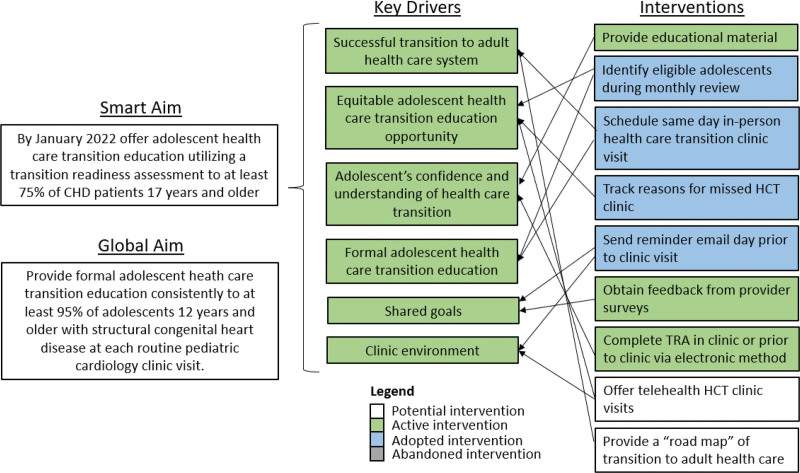
Introduction: We aim to implement healthcare transition (HCT) education for youth with congenital heart disease (CHD) and assess HCT preparedness for cardiac self-care.
Methods: An HCT clinic was implemented at an academic pediatric cardiology clinic for CHD youth 17 years of age and older. An educator used transition readiness assessment questionnaires and discussed HCT material. The percentage of eligible youth who received HCT education and the cause for missed occurrences were tracked. Plan-do-study-act cycles began in August 2020 to improve the number of youths reached. Secondary analyses assessed improvement differences among those without cardiac procedures or disabilities.
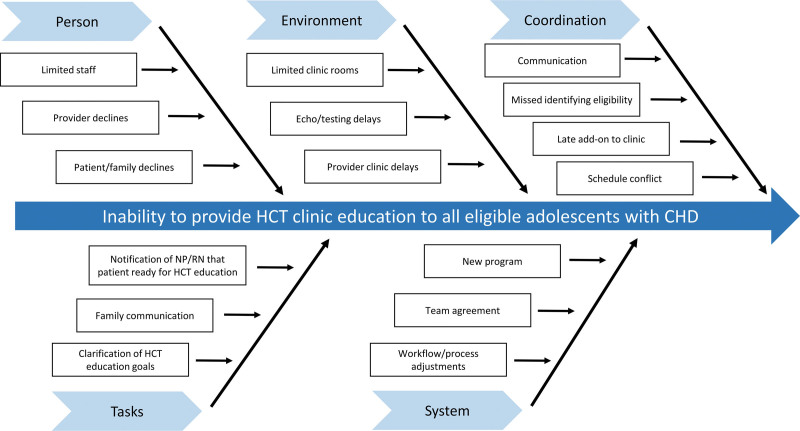
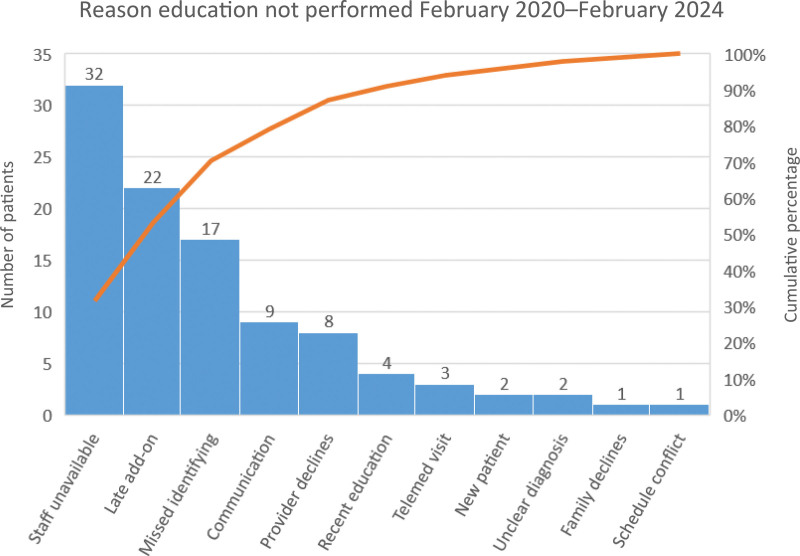
Results: HCT education provision improved from a mean of 38% to 73% in the 17-year and older age group by December 2022. Communication failure was the leading cause of missed visits in 2021 (30%), reduced to 0 by 2022 following plan-do-study-act cycles. Other missed HCT visits included clinic add-ons after screening, limited staff availability, and unidentified eligibility. Readiness assessments were similar for youth with and without prior cardiac procedures, for example, confidence in taking charge of their health care (P = 0.47) and moving to adult care (P = 0.22). Adolescents with disabilities were significantly less confident than those without disabilities in taking charge of their heart health care (6.3 versus 7.5, P = 0.04) and moving to adult care (4.9 versus 7.4, P < 0.001).
Conclusions: Implementation of a CHD HCT clinic improved successful education delivery. Provider engagement and clinic staffing are important for sustainability. HCT knowledge gaps exist for all adolescents, yet those with disabilities had the greatest deficits.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
