Impact of the 2022 pulmonary hypertension definition on haemodynamic classification and mortality in patients with aortic stenosis undergoing valve replacement.
Micha T Maeder, Lukas Weber, Susanne Pohle, Joannis Chronis, Florent Baty, Johannes Rigger, Martin Brutsche, Philipp Haager, Hans Rickli, Roman Brenner
{"title":"Impact of the 2022 pulmonary hypertension definition on haemodynamic classification and mortality in patients with aortic stenosis undergoing valve replacement.","authors":"Micha T Maeder, Lukas Weber, Susanne Pohle, Joannis Chronis, Florent Baty, Johannes Rigger, Martin Brutsche, Philipp Haager, Hans Rickli, Roman Brenner","doi":"10.1093/ehjopen/oeae037","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>With the 2022 pulmonary hypertension (PH) definition, the mean pulmonary artery pressure (mPAP) threshold for any PH was lowered from ≥25 to >20 mmHg, and the pulmonary vascular resistance (PVR) value to differentiate between isolated post-capillary PH (IpcPH) and combined pre- and post-capillary PH (CpcPH) was reduced from >3 Wood units (WU) to >2 WU. We assessed the impact of this change in the PH definition in aortic stenosis (AS) patients undergoing aortic valve replacement (AVR).</p><p><strong>Methods and results: </strong>Severe AS patients (<i>n</i> = 503) undergoing pre-AVR cardiac heart catheterization were classified according to both the 2015 and 2022 definitions. The post-AVR mortality [median follow-up 1348 (interquartile range 948-1885) days] was assessed. According to the 2015 definition, 219 (44% of the entire population) patients had PH: 63 (29%) CpcPH, 125 (57%) IpcPH, and 31 (14%) pre-capillary PH. According to the 2022 definition, 321 (+47%) patients were diagnosed with PH, and 156 patients (31%) were re-classified: 26 patients from no PH to IpcPH, 38 from no PH to pre-capillary PH, 38 from no PH to unclassified PH, 4 from pre-capillary PH to unclassified PH, and 50 from IpcPH to CpcPH (CpcPH: +79%). With both definitions, only the CpcPH patients displayed increased mortality (hazard ratios ≈ 4). Among the PH-defining haemodynamic components, PVR was the strongest predictor of death.</p><p><strong>Conclusion: </strong>In severe AS, the application of the 2022 PH definition results in a substantially higher number of patients with any PH as well as CpcPH. With either definition, CpcPH patients have a significantly increased post-AVR mortality.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"4 3","pages":"oeae037"},"PeriodicalIF":0.0000,"publicationDate":"2024-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11135639/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeae037","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
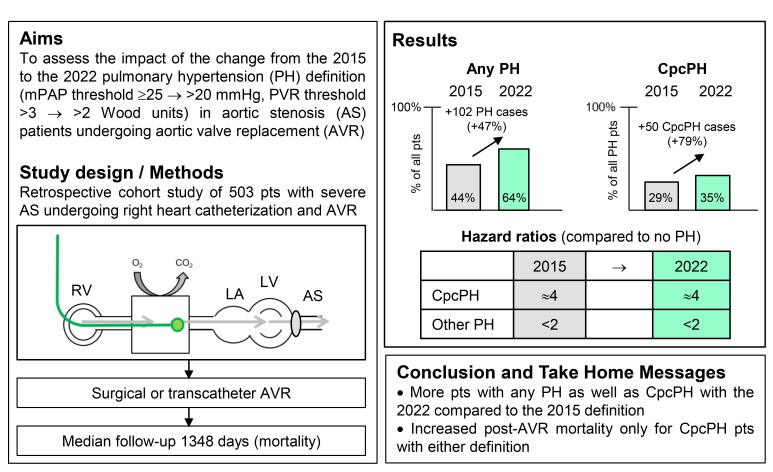
Aims: With the 2022 pulmonary hypertension (PH) definition, the mean pulmonary artery pressure (mPAP) threshold for any PH was lowered from ≥25 to >20 mmHg, and the pulmonary vascular resistance (PVR) value to differentiate between isolated post-capillary PH (IpcPH) and combined pre- and post-capillary PH (CpcPH) was reduced from >3 Wood units (WU) to >2 WU. We assessed the impact of this change in the PH definition in aortic stenosis (AS) patients undergoing aortic valve replacement (AVR).
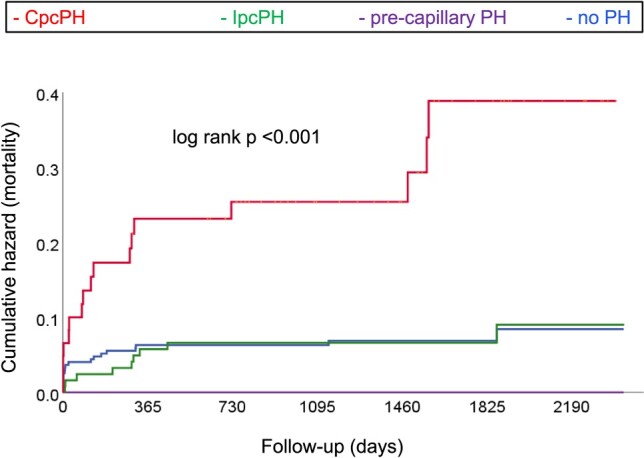
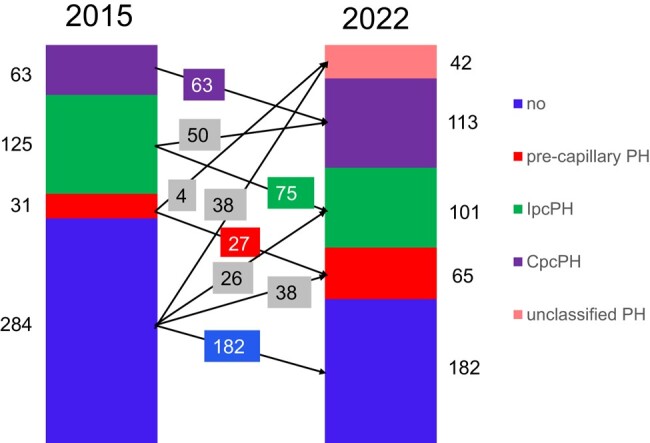
Methods and results: Severe AS patients (n = 503) undergoing pre-AVR cardiac heart catheterization were classified according to both the 2015 and 2022 definitions. The post-AVR mortality [median follow-up 1348 (interquartile range 948-1885) days] was assessed. According to the 2015 definition, 219 (44% of the entire population) patients had PH: 63 (29%) CpcPH, 125 (57%) IpcPH, and 31 (14%) pre-capillary PH. According to the 2022 definition, 321 (+47%) patients were diagnosed with PH, and 156 patients (31%) were re-classified: 26 patients from no PH to IpcPH, 38 from no PH to pre-capillary PH, 38 from no PH to unclassified PH, 4 from pre-capillary PH to unclassified PH, and 50 from IpcPH to CpcPH (CpcPH: +79%). With both definitions, only the CpcPH patients displayed increased mortality (hazard ratios ≈ 4). Among the PH-defining haemodynamic components, PVR was the strongest predictor of death.
Conclusion: In severe AS, the application of the 2022 PH definition results in a substantially higher number of patients with any PH as well as CpcPH. With either definition, CpcPH patients have a significantly increased post-AVR mortality.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
