It is unclear whether treatment early after onset in bipolar disorder may improve the long-term illness course. The early intervention in affective disorders (EIA) randomised controlled trial found that 2-years treatment in a specialised mood disorder clinic combining evidence-based pharmacological treatment with group psychoeducation improved clinical outcomes compared with standard treatment in patients with bipolar disorder discharged after their 1st, 2nd, or 3rd hospital admission. We aimed to assess the 16 years long-term outcomes after randomisation of the participants in the EIA trial.
Data were obtained by linking nation-wide Danish population-based registers. All 158 participants of the EIA trial (Trial Registration Number NCT00253071) were followed from time of randomisation (2005–2009) to end of study (31 December 2021). The primary outcome was risk of psychiatric readmission. Secondary outcomes were total admissions and costs, medication use, intentional self-harm or suicide attempt or suicide, and socio-economic measures.
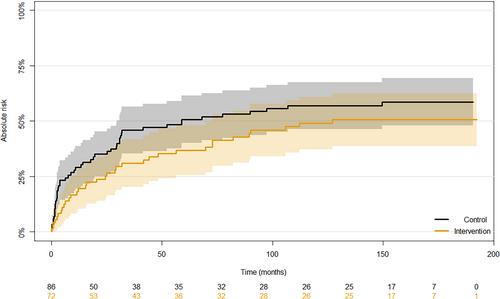
The absolute mean risk of psychiatric readmission was 49.3% in the intervention group and 59.8% in the control group, with no statistically significant difference between the groups (b = −0.10, 95% CI: −0.26 to 0.047, p = 0.18). Compared with the control group, patients in the intervention group had numerically fewer total admission days (mean (SD) 44 (77) versus 62 (109)), lower total cost of psychiatric hospital admissions and hospital-based outpatient visits (mean (SD) 22,001 (36793) euros versus 29,822 (52671) euros) and higher use of lithium and antipsychotics, but the differences were not statistically significant. Fewer patients in the intervention group had an event of intentional self-harm or suicide attempt or suicide during follow-up (OR 0.25, 95% CI: 0.15–0.40, p < 0.001) compared with the control group and more patients in the intervention group used antiepileptics (OR 2.21, 95% CI: 1.08–4.60, p = 0.031).
Analyses of very long-term outcomes of the EIA trial may potentially indicate a beneficial effect of the intervention at the long term but were likely underpowered to detect a more subtle effect and for most outcomes the differences between groups were not statistically significant.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
