Ahmad N Fasseeh, Nada Korra, Baher Elezbawy, Amal S Sedrak, Mary Gamal, Randa Eldessouki, Mariam Eldebeiky, Mohsen George, Ahmed Seyam, Asmaa Abourawash, Ahmed Y Khalifa, Mayada Shaheen, Sherif Abaza, Zoltán Kaló
{"title":"Framework for developing cost-effectiveness analysis threshold: the case of Egypt.","authors":"Ahmad N Fasseeh, Nada Korra, Baher Elezbawy, Amal S Sedrak, Mary Gamal, Randa Eldessouki, Mariam Eldebeiky, Mohsen George, Ahmed Seyam, Asmaa Abourawash, Ahmed Y Khalifa, Mayada Shaheen, Sherif Abaza, Zoltán Kaló","doi":"10.1186/s42506-024-00159-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cost-effectiveness analyses rarely offer useful insights to policy decisions unless their results are compared against a benchmark threshold. The cost-effectiveness threshold (CET) represents the maximum acceptable monetary value for achieving a unit of health gain. This study aimed to identify CET values on a global scale, provide an overview of using multiple CETs, and propose a country-specific CET framework specifically tailored for Egypt. The proposed framework aims to consider the globally identified CETs, analyze global trends, and consider the local structure of Egypt's healthcare system.</p><p><strong>Methods: </strong>We conducted a literature review to identify CET values, with a particular focus on understanding the basis of differentiation when multiple thresholds are present. CETs of different countries were reviewed from secondary sources. Additionally, we assembled an expert panel to develop a national CET framework in Egypt and propose an initial design. This was followed by a multistakeholder workshop, bringing together representatives of different governmental bodies to vote on the threshold value and finalize the recommended framework.</p><p><strong>Results: </strong>The average CET, expressed as a percentage of the gross domestic product (GDP) per capita across all countries, was 135%, with a range of 21 to 300%. Interestingly, while the absolute value of CET increased with a country's income level, the average CET/GDP per capita showed an inverse relationship. Some countries applied multiple thresholds based on disease severity or rarity. In the case of Egypt, the consensus workshop recommended a threshold ranging from one to three times the GDP per capita, taking into account the incremental relative quality-adjusted life years (QALY) gain. For orphan medicines, a CET multiplier between 1.5 and 3.0, based on the disease rarity, was recommended. A two-times multiplier was proposed for the private reimbursement threshold compared to the public threshold.</p><p><strong>Conclusion: </strong>The CET values in most countries appear to be closely related to the GDP per capita. Higher-income countries tend to use a lower threshold as a percentage of their GDP per capita, contrasted with lower-income countries. In Egypt, experts opted for a multiple CET framework to assess the value of health technologies in terms of reimbursement and pricing.</p>","PeriodicalId":22819,"journal":{"name":"The Journal of the Egyptian Public Health Association","volume":"99 1","pages":"12"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11144683/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Journal of the Egyptian Public Health Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42506-024-00159-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Nursing","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cost-effectiveness analyses rarely offer useful insights to policy decisions unless their results are compared against a benchmark threshold. The cost-effectiveness threshold (CET) represents the maximum acceptable monetary value for achieving a unit of health gain. This study aimed to identify CET values on a global scale, provide an overview of using multiple CETs, and propose a country-specific CET framework specifically tailored for Egypt. The proposed framework aims to consider the globally identified CETs, analyze global trends, and consider the local structure of Egypt's healthcare system.
Methods: We conducted a literature review to identify CET values, with a particular focus on understanding the basis of differentiation when multiple thresholds are present. CETs of different countries were reviewed from secondary sources. Additionally, we assembled an expert panel to develop a national CET framework in Egypt and propose an initial design. This was followed by a multistakeholder workshop, bringing together representatives of different governmental bodies to vote on the threshold value and finalize the recommended framework.
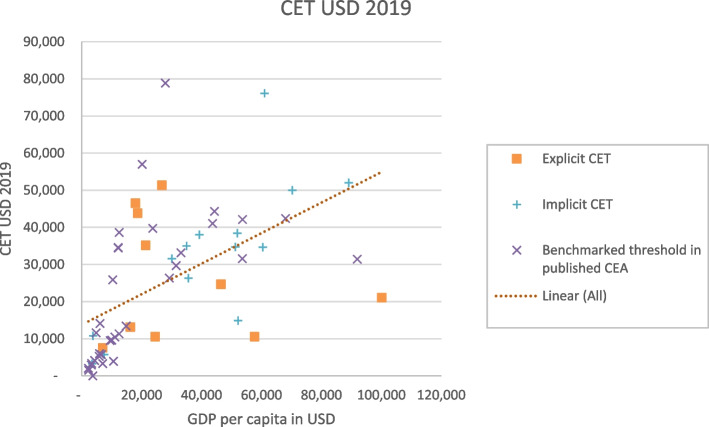
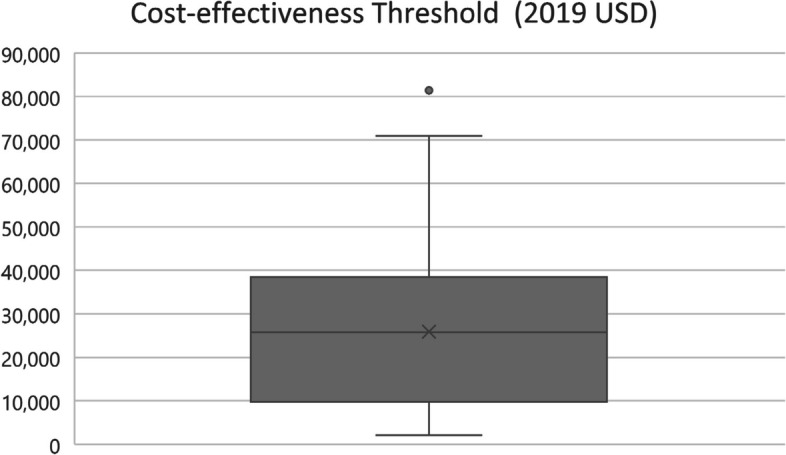
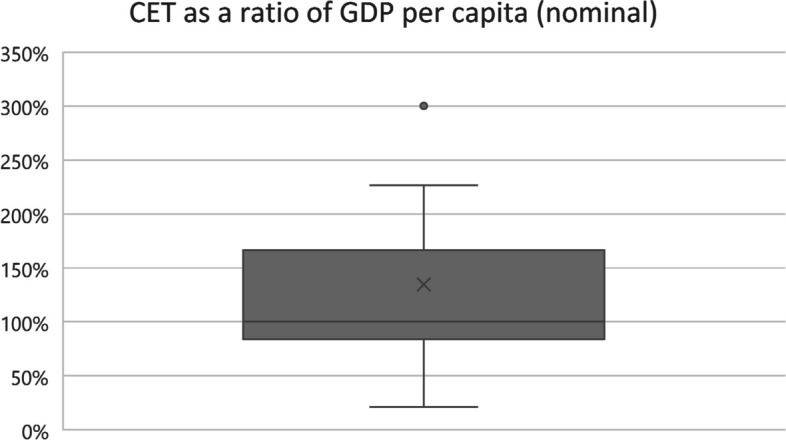
Results: The average CET, expressed as a percentage of the gross domestic product (GDP) per capita across all countries, was 135%, with a range of 21 to 300%. Interestingly, while the absolute value of CET increased with a country's income level, the average CET/GDP per capita showed an inverse relationship. Some countries applied multiple thresholds based on disease severity or rarity. In the case of Egypt, the consensus workshop recommended a threshold ranging from one to three times the GDP per capita, taking into account the incremental relative quality-adjusted life years (QALY) gain. For orphan medicines, a CET multiplier between 1.5 and 3.0, based on the disease rarity, was recommended. A two-times multiplier was proposed for the private reimbursement threshold compared to the public threshold.
Conclusion: The CET values in most countries appear to be closely related to the GDP per capita. Higher-income countries tend to use a lower threshold as a percentage of their GDP per capita, contrasted with lower-income countries. In Egypt, experts opted for a multiple CET framework to assess the value of health technologies in terms of reimbursement and pricing.
背景:除非将成本效益分析结果与基准阈值进行比较,否则成本效益分析很少能为政策决策提供有用的见解。成本效益阈值 (CET) 代表了实现单位健康收益的最大可接受货币价值。本研究旨在确定全球范围内的 CET 值,概述多种 CET 的使用情况,并提出一个专为埃及量身定制的国别 CET 框架。建议的框架旨在考虑全球范围内确定的 CET,分析全球趋势,并考虑埃及医疗保健系统的本地结构:方法:我们进行了文献综述,以确定 CET 值,尤其侧重于了解存在多个阈值时的区分依据。我们从二手资料中查阅了不同国家的 CET。此外,我们还组建了一个专家小组,以制定埃及国家 CET 框架并提出初步设计。随后,我们召开了一次多方利益相关者研讨会,汇集了不同政府机构的代表,就阈值进行投票,并最终确定了建议的框架:以人均国内生产总值 (GDP) 的百分比表示,所有国家的平均 CET 为 135%,范围在 21% 到 300% 之间。有趣的是,虽然 CET 的绝对值随着国家收入水平的提高而增加,但平均 CET/GDP 人均值却呈反比关系。一些国家根据疾病的严重程度或罕见程度采用了多种阈值。就埃及而言,考虑到相对质量调整生命年(QALY)的增量,共识研讨会建议将阈值定为人均 GDP 的 1 到 3 倍。对于孤儿药,根据疾病的罕见程度,建议采用 1.5 至 3.0 倍的 CET 乘数。结论:大多数国家的 CET 值似乎与人均国内生产总值密切相关。与低收入国家相比,高收入国家往往采用较低的阈值(占人均国内生产总值的百分比)。在埃及,专家们选择了多重 CET 框架来评估医疗技术在报销和定价方面的价值。
期刊介绍:
The journal accepts papers of original research which are not being considered for publication elsewhere and which contribute to the advancement of knowledge of Public Health at large


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
