Murat Kara, Eren Erdogdu, Salih Duman, Gulnar Fatalizade, Berker Ozkan, Alper Toker
{"title":"Potential Survival Benefit of Upfront Surgery for Lung Tumors Unconfirmed but Highly Suspicious for Stage I Lung Cancer.","authors":"Murat Kara, Eren Erdogdu, Salih Duman, Gulnar Fatalizade, Berker Ozkan, Alper Toker","doi":"10.5090/jcs.23.166","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with early-stage lung tumors that are highly suspicious for malignancy typically undergo a preoperative diagnostic workup, primarily through bronchoscopy or transthoracic biopsy. Those without a preoperative diagnosis may alternatively be treated with upfront surgery, contingent upon the potential for intraoperative diagnosis. Previous studies have yielded conflicting results regarding the impact of upfront surgery on the survival of these patients. Our study aimed to elucidate the effect of upfront surgery on the survival outcomes of patients undergoing surgery for early-stage lung cancer without a preoperative diagnosis.</p><p><strong>Methods: </strong>We analyzed the survival rate of 158 consecutive patients who underwent pulmonary resection for stage I lung cancer, either with or without a preoperative diagnosis.</p><p><strong>Results: </strong>A total of 86 patients (54%) underwent upfront surgery. This approach positively impacted both disease-free survival (p=0.031) and overall survival (p=0.017). However, no significant differences were observed across subgroups based on sex, smoking status, forced expiratory volume in 1 second, histologic tumor size, or histologic subtype. Univariate analysis identified upfront surgery (p=0.020), age (p=0.002), maximum standardized uptake value (SUVmax) exceeding 7 (p=0.001), and histological tumor size greater than 20 mm (p=0.009) as independent predictors. However, multivariate analysis indicated that only SUVmax greater than 7 (p=0.011) was a significant predictor of unfavorable survival.</p><p><strong>Conclusion: </strong>Upfront surgery does not appear to confer a survival advantage in patients with stage I lung cancer undergoing surgical intervention.</p>","PeriodicalId":34499,"journal":{"name":"Journal of Chest Surgery","volume":" ","pages":"440-446"},"PeriodicalIF":1.0000,"publicationDate":"2024-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11392711/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Chest Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/jcs.23.166","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/5 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with early-stage lung tumors that are highly suspicious for malignancy typically undergo a preoperative diagnostic workup, primarily through bronchoscopy or transthoracic biopsy. Those without a preoperative diagnosis may alternatively be treated with upfront surgery, contingent upon the potential for intraoperative diagnosis. Previous studies have yielded conflicting results regarding the impact of upfront surgery on the survival of these patients. Our study aimed to elucidate the effect of upfront surgery on the survival outcomes of patients undergoing surgery for early-stage lung cancer without a preoperative diagnosis.
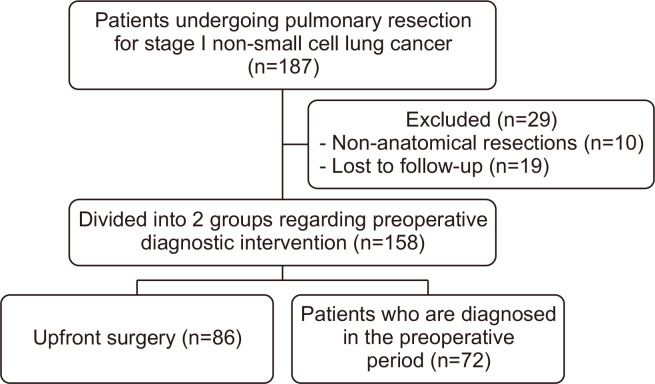
Methods: We analyzed the survival rate of 158 consecutive patients who underwent pulmonary resection for stage I lung cancer, either with or without a preoperative diagnosis.
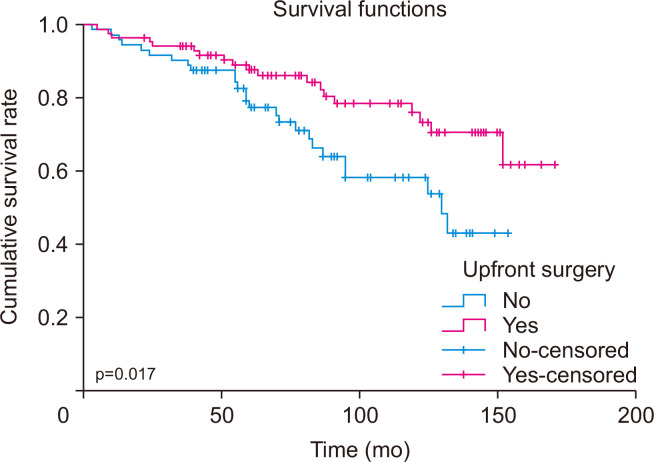
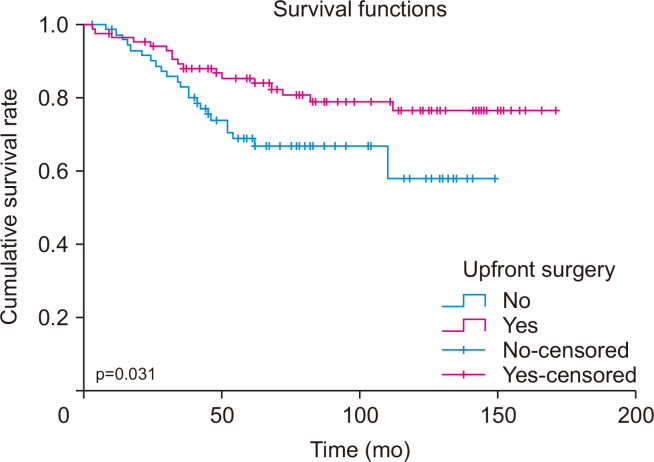
Results: A total of 86 patients (54%) underwent upfront surgery. This approach positively impacted both disease-free survival (p=0.031) and overall survival (p=0.017). However, no significant differences were observed across subgroups based on sex, smoking status, forced expiratory volume in 1 second, histologic tumor size, or histologic subtype. Univariate analysis identified upfront surgery (p=0.020), age (p=0.002), maximum standardized uptake value (SUVmax) exceeding 7 (p=0.001), and histological tumor size greater than 20 mm (p=0.009) as independent predictors. However, multivariate analysis indicated that only SUVmax greater than 7 (p=0.011) was a significant predictor of unfavorable survival.
Conclusion: Upfront surgery does not appear to confer a survival advantage in patients with stage I lung cancer undergoing surgical intervention.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
