{"title":"Enhancing surgical precision in early-stage non-small cell lung cancer: A novel approach through temporary pulmonary vascular occlusion.","authors":"Yan Zhao, Bin You, Hui Li","doi":"10.1111/1759-7714.15388","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To evaluate a novel intraoperative localization technique utilizing temporary pulmonary arteriovenous occlusion for enhancing the precision of sublobar resections in early-stage NSCLC.</p><p><strong>Methods: </strong>Conducted from January to November 2023, this study involved 140 patients. During the surgery, key pulmonary vessels were identified using preoperative three-dimensional (3D) imaging and temporarily occluded with noninvasive clamps to isolate the target lung segment. Following vascular occlusion, indocyanine green (ICG) was administered intravenously to precisely delineate the resection margins. After visually confirming the marked areas, the clamps were released, and a targeted partial resection was performed on the delineated segment. Surgical data, including operation times, surgical margins, and hospitalization costs, were collected and compared with those from a historical control group of 110 patients who underwent traditional pulmonary wedge resections.</p><p><strong>Results: </strong>In the study group, the median surgical margin achieved was 16 mm, which was statistically significant compared to 15 mm in the control group (p < 0.05). Operation times were reduced to an average of 58.43 ± 12.962 min, showing a decrease from the control group's average of 69.50 ± 17.544 min (p < 0.05). Hospitalization costs were also lower, averaging $4772.98 ± 624.339 for the study group versus $5161.34 ± 856.336 for the control group (p < 0.05). Patient safety was maintained with no increase in surgical complications.</p><p><strong>Conclusion: </strong>The technique, leveraging temporary pulmonary arteriovenous occlusion, offered a significant advancement in the surgical treatment of peripheral early-stage NSCLC. It reduced operation time and lowered overall surgical costs. This method represented a promising alternative to traditional surgical approaches.</p>","PeriodicalId":23338,"journal":{"name":"Thoracic Cancer","volume":" ","pages":"1582-1589"},"PeriodicalIF":2.3000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11246783/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thoracic Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/1759-7714.15388","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/4 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: To evaluate a novel intraoperative localization technique utilizing temporary pulmonary arteriovenous occlusion for enhancing the precision of sublobar resections in early-stage NSCLC.
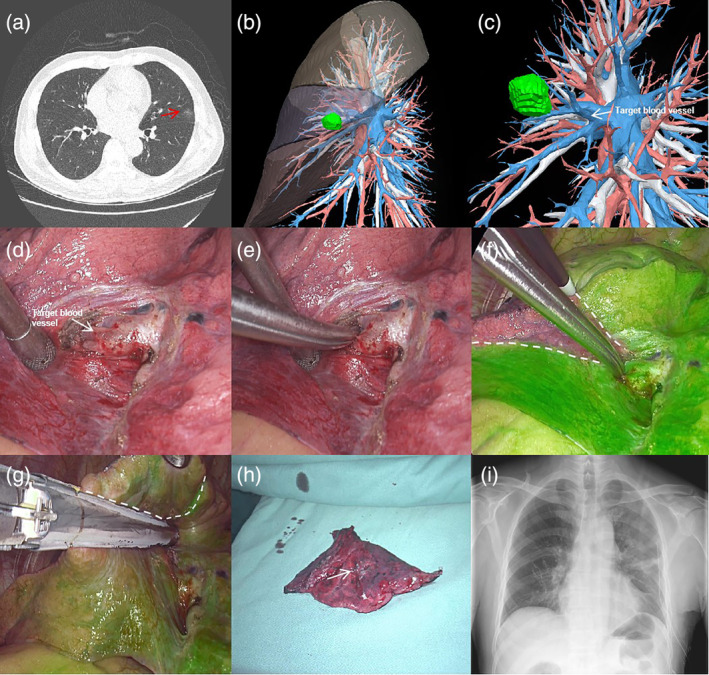
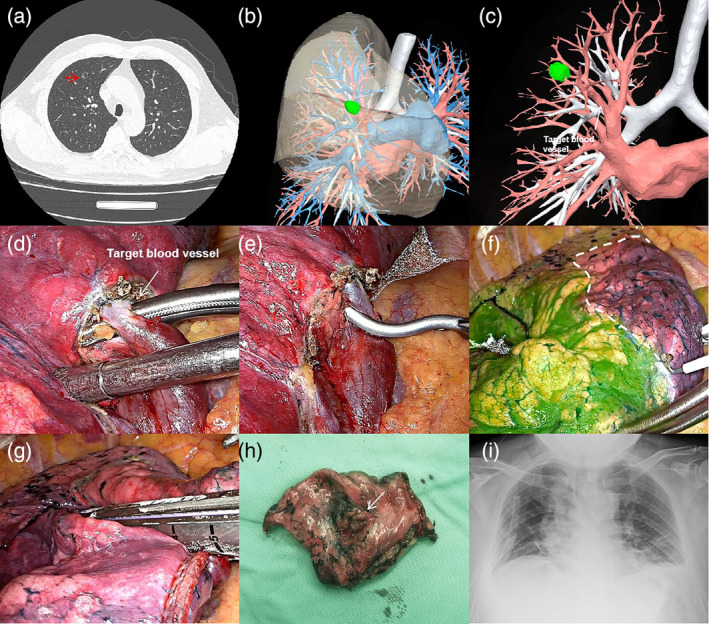
Methods: Conducted from January to November 2023, this study involved 140 patients. During the surgery, key pulmonary vessels were identified using preoperative three-dimensional (3D) imaging and temporarily occluded with noninvasive clamps to isolate the target lung segment. Following vascular occlusion, indocyanine green (ICG) was administered intravenously to precisely delineate the resection margins. After visually confirming the marked areas, the clamps were released, and a targeted partial resection was performed on the delineated segment. Surgical data, including operation times, surgical margins, and hospitalization costs, were collected and compared with those from a historical control group of 110 patients who underwent traditional pulmonary wedge resections.
Results: In the study group, the median surgical margin achieved was 16 mm, which was statistically significant compared to 15 mm in the control group (p < 0.05). Operation times were reduced to an average of 58.43 ± 12.962 min, showing a decrease from the control group's average of 69.50 ± 17.544 min (p < 0.05). Hospitalization costs were also lower, averaging $4772.98 ± 624.339 for the study group versus $5161.34 ± 856.336 for the control group (p < 0.05). Patient safety was maintained with no increase in surgical complications.
Conclusion: The technique, leveraging temporary pulmonary arteriovenous occlusion, offered a significant advancement in the surgical treatment of peripheral early-stage NSCLC. It reduced operation time and lowered overall surgical costs. This method represented a promising alternative to traditional surgical approaches.
期刊介绍:
Thoracic Cancer aims to facilitate international collaboration and exchange of comprehensive and cutting-edge information on basic, translational, and applied clinical research in lung cancer, esophageal cancer, mediastinal cancer, breast cancer and other thoracic malignancies. Prevention, treatment and research relevant to Asia-Pacific is a focus area, but submissions from all regions are welcomed. The editors encourage contributions relevant to prevention, general thoracic surgery, medical oncology, radiology, radiation medicine, pathology, basic cancer research, as well as epidemiological and translational studies in thoracic cancer. Thoracic Cancer is the official publication of the Chinese Society of Lung Cancer, International Chinese Society of Thoracic Surgery and is endorsed by the Korean Association for the Study of Lung Cancer and the Hong Kong Cancer Therapy Society.
The Journal publishes a range of article types including: Editorials, Invited Reviews, Mini Reviews, Original Articles, Clinical Guidelines, Technological Notes, Imaging in thoracic cancer, Meeting Reports, Case Reports, Letters to the Editor, Commentaries, and Brief Reports.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
