Linda Zheng Pharm.D., Tiffany Pon Pharm.D., Sarah Bajorek Pharm.D., Kathie Le Pharm.D., Rebecca Hluhanich Pharm.D., Yunyi Ren M.S., Machelle Wilson Ph.D.
{"title":"Impact of pharmacist-led discharge medication reconciliation on error and patient harm prevention at a large academic medical center","authors":"Linda Zheng Pharm.D., Tiffany Pon Pharm.D., Sarah Bajorek Pharm.D., Kathie Le Pharm.D., Rebecca Hluhanich Pharm.D., Yunyi Ren M.S., Machelle Wilson Ph.D.","doi":"10.1002/jac5.1980","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Medication errors during hospital discharge can lead to adverse outcomes, medication-related readmissions, and increased health care costs. Pharmacist-led medication reconciliation at discharge is a potential solution to mitigate poor outcomes and optimize medication safety.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>This study aimed to quantify medication errors identified at discharge and characterize the severity of patient harm prevented following pharmacist-led discharge medication reconciliation. Cost avoidance analysis was conducted to determine its associated financial impact.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients, who were discharged from an adult internal medicine service during October 2022, were included in this one-month pilot prospective quality improvement study. The number of errors at discharge were documented, categorized by type, and adjudicated for severity of potential harm. Error severity was classified based on a modified National Coordinating Council for Medication Error Reporting and Prevention Medication Error Index. Cost avoidance was calculated based on whether each error would have resulted in additional medical encounters and length of stay.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Thirty-one patients were included in the analysis. Forty errors were identified by pharmacist-led medication reconciliation at discharge, with a mean of 1.3 ± 1.9 errors per patient and 68% of patients having at least one error. The most common errors were duplication of therapy (25%) and medication access barriers at discharge (25%). The severity of errors included low (22.5%), serious (75%), and life-threatening harm (2.5%). Thirty-five percent of errors could have led to emergency visits or hospital readmissions. The estimated total cost for errors was $25 600. Pharmacist labor cost for reconciliation was $816. Cost avoidance was $24 784 from the 14 errors at discharge that could have resulted in additional emergency or inpatient visits.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Pharmacist-led medication reconciliation at discharge may prevent harm from reaching patients, decrease cost from unnecessary health encounters, and stop the error from continuing across transitions of care.</p>\n </section>\n </div>","PeriodicalId":73966,"journal":{"name":"Journal of the American College of Clinical Pharmacy : JACCP","volume":"7 8","pages":"787-794"},"PeriodicalIF":1.5000,"publicationDate":"2024-06-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jac5.1980","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Clinical Pharmacy : JACCP","FirstCategoryId":"1085","ListUrlMain":"https://accpjournals.onlinelibrary.wiley.com/doi/10.1002/jac5.1980","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
Medication errors during hospital discharge can lead to adverse outcomes, medication-related readmissions, and increased health care costs. Pharmacist-led medication reconciliation at discharge is a potential solution to mitigate poor outcomes and optimize medication safety.
Objectives
This study aimed to quantify medication errors identified at discharge and characterize the severity of patient harm prevented following pharmacist-led discharge medication reconciliation. Cost avoidance analysis was conducted to determine its associated financial impact.
Methods
Patients, who were discharged from an adult internal medicine service during October 2022, were included in this one-month pilot prospective quality improvement study. The number of errors at discharge were documented, categorized by type, and adjudicated for severity of potential harm. Error severity was classified based on a modified National Coordinating Council for Medication Error Reporting and Prevention Medication Error Index. Cost avoidance was calculated based on whether each error would have resulted in additional medical encounters and length of stay.
Results
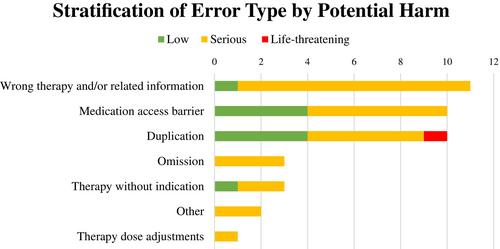
Thirty-one patients were included in the analysis. Forty errors were identified by pharmacist-led medication reconciliation at discharge, with a mean of 1.3 ± 1.9 errors per patient and 68% of patients having at least one error. The most common errors were duplication of therapy (25%) and medication access barriers at discharge (25%). The severity of errors included low (22.5%), serious (75%), and life-threatening harm (2.5%). Thirty-five percent of errors could have led to emergency visits or hospital readmissions. The estimated total cost for errors was $25 600. Pharmacist labor cost for reconciliation was $816. Cost avoidance was $24 784 from the 14 errors at discharge that could have resulted in additional emergency or inpatient visits.
Conclusion
Pharmacist-led medication reconciliation at discharge may prevent harm from reaching patients, decrease cost from unnecessary health encounters, and stop the error from continuing across transitions of care.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
