Suzana Măceș Piele, Silviu Daniel Preda, Ștefan Pătrașcu, Stylliani Laskou, Konstantinos Sapalidis, Daniela Dumitrescu, Valeriu Șurlin
{"title":"Indication and Timing of Cholecystectomy in Acute Biliary Pancreatitis - Systematic Review.","authors":"Suzana Măceș Piele, Silviu Daniel Preda, Ștefan Pătrașcu, Stylliani Laskou, Konstantinos Sapalidis, Daniela Dumitrescu, Valeriu Șurlin","doi":"10.12865/CHSJ.50.01.16","DOIUrl":null,"url":null,"abstract":"<p><p>Acute biliary pancreatitis (ABP) poses significant challenges in determining the optimal timing and approach for cholecystectomy, particularly in mild, moderately severe, and severe forms. This article reviews the existing literature on cholecystectomy timing and its impact on outcomes in ABP. A systematic literature search yielded 41 relevant articles from PubMed and Scopus databases. In mild ABP, early cholecystectomy within 72 hours of onset is increasingly favoured due to reduced technical difficulty and lower risk of recurrent pancreatitis. Conversely, delayed cholecystectomy, although traditionally practiced, may lead to higher recurrence rates and prolonged hospital stays. For moderate severe ABP, evidence remains limited, but early cholecystectomy appears to decrease hospital stay without increasing perioperative complications. In severe ABP, consensus suggests delaying cholecystectomy until peripancreatic collections resolve, typically 6 to 10 weeks post-onset, to minimize surgical morbidity. The role of endoscopic retrograde cholangiopancreatography (ERCP) alongside cholecystectomy remains contentious, with guidelines recommending its use in specific scenarios such as cholangitis or biliary obstruction. However, routine ERCP in mild ABP lacks robust evidence and may increase complications. Challenges persist regarding the management of residual choledocholithiasis post-ABP, highlighting the need for improved diagnostic criteria and management protocols. Overall, this review underscores the evolving landscape of cholecystectomy timing in ABP and provides insights into current best practices and areas for future research.</p>","PeriodicalId":93963,"journal":{"name":"Current health sciences journal","volume":"50 1","pages":"125-132"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11151952/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current health sciences journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12865/CHSJ.50.01.16","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
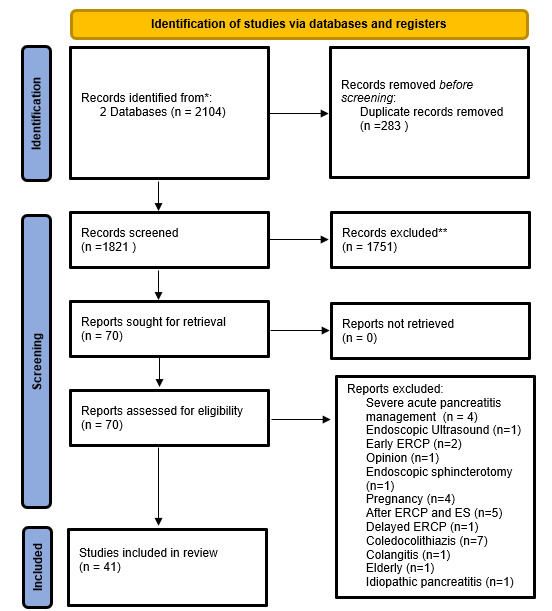
Acute biliary pancreatitis (ABP) poses significant challenges in determining the optimal timing and approach for cholecystectomy, particularly in mild, moderately severe, and severe forms. This article reviews the existing literature on cholecystectomy timing and its impact on outcomes in ABP. A systematic literature search yielded 41 relevant articles from PubMed and Scopus databases. In mild ABP, early cholecystectomy within 72 hours of onset is increasingly favoured due to reduced technical difficulty and lower risk of recurrent pancreatitis. Conversely, delayed cholecystectomy, although traditionally practiced, may lead to higher recurrence rates and prolonged hospital stays. For moderate severe ABP, evidence remains limited, but early cholecystectomy appears to decrease hospital stay without increasing perioperative complications. In severe ABP, consensus suggests delaying cholecystectomy until peripancreatic collections resolve, typically 6 to 10 weeks post-onset, to minimize surgical morbidity. The role of endoscopic retrograde cholangiopancreatography (ERCP) alongside cholecystectomy remains contentious, with guidelines recommending its use in specific scenarios such as cholangitis or biliary obstruction. However, routine ERCP in mild ABP lacks robust evidence and may increase complications. Challenges persist regarding the management of residual choledocholithiasis post-ABP, highlighting the need for improved diagnostic criteria and management protocols. Overall, this review underscores the evolving landscape of cholecystectomy timing in ABP and provides insights into current best practices and areas for future research.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
