Alban Gildas Comlan Zohoun, Tatiana Bagloagbodande, Axel Adanho, Romaric Massi, Bienvenu Houssou, Gnon Gourou Orou Guiwa, Justin Dèhoumon, Josiane Mehou, Ludovic Anani, Anne Vovor, Dorothée Kindegazard
{"title":"[Blood count abnormalities in the association of sickle cell disease and malaria in clinical hematology at the CNHU-HKM in Cotonou (Bénin)].","authors":"Alban Gildas Comlan Zohoun, Tatiana Bagloagbodande, Axel Adanho, Romaric Massi, Bienvenu Houssou, Gnon Gourou Orou Guiwa, Justin Dèhoumon, Josiane Mehou, Ludovic Anani, Anne Vovor, Dorothée Kindegazard","doi":"10.48327/mtsi.v4i1.2024.404","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Although a protective effect of hemoglobin S has been described, malaria has frequently been associated with increased morbidity and mortality in sickle cell disease patients in Africa. Various cytopenias are frequently found on the haemograms of these patients. In Benin, a malaria-endemic zone with a high prevalence of sickle cell disease, the aim of this study was to establish and compare the blood count profile according to hemoglobin type in the association of sickle cell disease and malaria.</p><p><strong>Material and method: </strong>This was a prospective descriptive study. It covered a 24-month period from October 2020 to October 2022. It included all patients with major sickle cell syndrome seen in clinical haematology and with a positive thick drop/parasite density, whatever the parasitaemia value. For each patient, a blood count was performed on the Sysmex XT 4000i machine, supplemented by a smear study after staining with May-Grunwald Giemsa. Data were analyzed using R 3.6.1 software.</p><p><strong>Results: </strong>Three hundred non-redundant cases with a positive thick smear were identified in sickle cell patients, including 208 SS homozygotes (69.3%) and 92 SC heterozygotes (30.7%). In contrast, there were 181 non-redundant cases with a negative thick smear, including 119 SS homozygotes (65.7%) and 62 SC heterozygotes (34.3%). Among subjects with a positive thick smear, the majority of patients (70%) exhibited clinical symptoms. Severe malaria was observed in 58% of the cases. The proportion of severe malaria was higher in SS homozygote patients than in double heterozygote SC patients (p < 0.0001). The mean parasite density was higher in SS individuals (4 320.7 ± 2 185 trophozoites/pL) compared to SC individuals (1 564.4 ± 1 221 trophozoites/pL; p < 0.0001). <i>Plasmodium falciparum</i> was the only species identified. The mean hemoglobin level in impaludated SS subjects was 6.1 g/dL, significantly lower than that in non-impaludated SS subjects (p < 0.0001). The average white blood cell count in impaludated SS subjects was 16.58 G/L, compared to 13.2 G/L in those with a negative thick smear (p < 0.0001). Twenty cases of thrombocytopenia were found in SS subjects with a positive thick smear, compared to 6 cases in those with a negative thick smear. As for SC subjects with a positive thick smear, the average hemoglobin levels and white blood cell counts were 9.8 g/dL and 10.63 G/L, respectively, compared to 11.27 g/dL and 7.3 G/L in SC subjects with a negative thick smear. Eighteen cases of thrombocytopenia were found in subjects with a positive thick smear, compared to 17 cases in those with a negative thick smear.</p><p><strong>Discussion: </strong>Sickle cell disease and malaria represent two major public health problems. However, contrary to popular belief, sickle cell disease is not immune to malaria infestation. Malaria is recognized as one of the main causes of morbidity and mortality in sickle cell patients, particularly children. In Benin, its association with sickle cell emergencies has already been reported.Our study found that malaria was predominantly associated with the homozygous SS form (p < 0.00001). Severe malaria was the most common clinical form. All malaria infestations in our series were due to <i>Plasmodium falciparum,</i> and parasitaemia was significantly higher in SS patients (p < 0.0001).The hematological profile of the association of sickle cell disease and malaria in homozygous SS individuals in our series showed characteristics of a normocytic normochromic anemia with neutrophil-predominant leukocytosis. Compared to non-malaria-infected SS individuals, there was a significant worsening of anemia, neutrophil-predominant leukocytosis, and a decrease in the average platelet count. In SC individuals, there was rather a microcytic normochromic regenerative anemia associated with neutrophil-predominant leukocytosis. Compared to non-malaria-infected SC individuals, there was a significant decrease in the rate of anemia and neutrophil-predominant leukocytosis. Anemia is a constant feature in homozygous sickle cell disease, and the low values recorded illustrate the hemolytic nature of malaria, especially in SS individuals, and the better tolerance of SC individuals. Furthermore, the low baseline hemoglobin levels make SS individuals more vulnerable to malaria-induced anemia compared to SC individuals. The observed leukocytosis is generally accompanied by reticulocytosis in the case of major sickle cell syndrome, which must be taken into account for result validation. It is the expression of compensatory bone marrow reaction to anemia and inflammatory mechanisms resulting from malaria infestation. Finally, thrombocytopenia was significantly more common in SC patients, even though they were adults living in malaria-endemic areas. Malaria can frequently induce thrombocytopenia through platelet consumption during the \"rosetting\" phenomenon. In SS patients, the effects of \"rosetting\" could be compensated for by the bone marrow stimulation induced by anemia. In our series with adult subjects living in an endemic area, thrombocytopenia is not a frequent biological disturbance. In a clinicalbiological context combining a systemic inflammatory response syndrome with anemia and neutrophil-predominant leukocytosis in a SS or SC sickle cell patient, the clinician should be able to consider malaria and confirm or rule out this diagnosis.</p>","PeriodicalId":101416,"journal":{"name":"Medecine tropicale et sante internationale","volume":"4 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11151902/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medecine tropicale et sante internationale","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.48327/mtsi.v4i1.2024.404","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/31 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Although a protective effect of hemoglobin S has been described, malaria has frequently been associated with increased morbidity and mortality in sickle cell disease patients in Africa. Various cytopenias are frequently found on the haemograms of these patients. In Benin, a malaria-endemic zone with a high prevalence of sickle cell disease, the aim of this study was to establish and compare the blood count profile according to hemoglobin type in the association of sickle cell disease and malaria.
Material and method: This was a prospective descriptive study. It covered a 24-month period from October 2020 to October 2022. It included all patients with major sickle cell syndrome seen in clinical haematology and with a positive thick drop/parasite density, whatever the parasitaemia value. For each patient, a blood count was performed on the Sysmex XT 4000i machine, supplemented by a smear study after staining with May-Grunwald Giemsa. Data were analyzed using R 3.6.1 software.
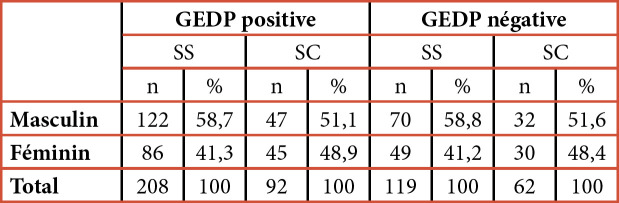
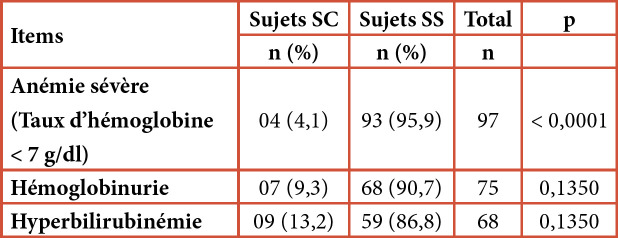
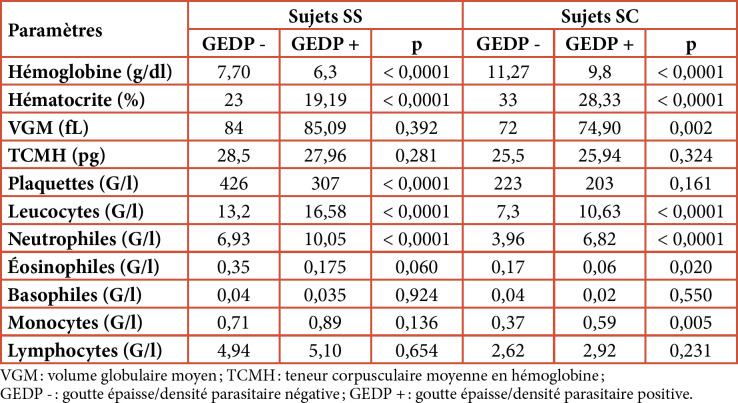
Results: Three hundred non-redundant cases with a positive thick smear were identified in sickle cell patients, including 208 SS homozygotes (69.3%) and 92 SC heterozygotes (30.7%). In contrast, there were 181 non-redundant cases with a negative thick smear, including 119 SS homozygotes (65.7%) and 62 SC heterozygotes (34.3%). Among subjects with a positive thick smear, the majority of patients (70%) exhibited clinical symptoms. Severe malaria was observed in 58% of the cases. The proportion of severe malaria was higher in SS homozygote patients than in double heterozygote SC patients (p < 0.0001). The mean parasite density was higher in SS individuals (4 320.7 ± 2 185 trophozoites/pL) compared to SC individuals (1 564.4 ± 1 221 trophozoites/pL; p < 0.0001). Plasmodium falciparum was the only species identified. The mean hemoglobin level in impaludated SS subjects was 6.1 g/dL, significantly lower than that in non-impaludated SS subjects (p < 0.0001). The average white blood cell count in impaludated SS subjects was 16.58 G/L, compared to 13.2 G/L in those with a negative thick smear (p < 0.0001). Twenty cases of thrombocytopenia were found in SS subjects with a positive thick smear, compared to 6 cases in those with a negative thick smear. As for SC subjects with a positive thick smear, the average hemoglobin levels and white blood cell counts were 9.8 g/dL and 10.63 G/L, respectively, compared to 11.27 g/dL and 7.3 G/L in SC subjects with a negative thick smear. Eighteen cases of thrombocytopenia were found in subjects with a positive thick smear, compared to 17 cases in those with a negative thick smear.
Discussion: Sickle cell disease and malaria represent two major public health problems. However, contrary to popular belief, sickle cell disease is not immune to malaria infestation. Malaria is recognized as one of the main causes of morbidity and mortality in sickle cell patients, particularly children. In Benin, its association with sickle cell emergencies has already been reported.Our study found that malaria was predominantly associated with the homozygous SS form (p < 0.00001). Severe malaria was the most common clinical form. All malaria infestations in our series were due to Plasmodium falciparum, and parasitaemia was significantly higher in SS patients (p < 0.0001).The hematological profile of the association of sickle cell disease and malaria in homozygous SS individuals in our series showed characteristics of a normocytic normochromic anemia with neutrophil-predominant leukocytosis. Compared to non-malaria-infected SS individuals, there was a significant worsening of anemia, neutrophil-predominant leukocytosis, and a decrease in the average platelet count. In SC individuals, there was rather a microcytic normochromic regenerative anemia associated with neutrophil-predominant leukocytosis. Compared to non-malaria-infected SC individuals, there was a significant decrease in the rate of anemia and neutrophil-predominant leukocytosis. Anemia is a constant feature in homozygous sickle cell disease, and the low values recorded illustrate the hemolytic nature of malaria, especially in SS individuals, and the better tolerance of SC individuals. Furthermore, the low baseline hemoglobin levels make SS individuals more vulnerable to malaria-induced anemia compared to SC individuals. The observed leukocytosis is generally accompanied by reticulocytosis in the case of major sickle cell syndrome, which must be taken into account for result validation. It is the expression of compensatory bone marrow reaction to anemia and inflammatory mechanisms resulting from malaria infestation. Finally, thrombocytopenia was significantly more common in SC patients, even though they were adults living in malaria-endemic areas. Malaria can frequently induce thrombocytopenia through platelet consumption during the "rosetting" phenomenon. In SS patients, the effects of "rosetting" could be compensated for by the bone marrow stimulation induced by anemia. In our series with adult subjects living in an endemic area, thrombocytopenia is not a frequent biological disturbance. In a clinicalbiological context combining a systemic inflammatory response syndrome with anemia and neutrophil-predominant leukocytosis in a SS or SC sickle cell patient, the clinician should be able to consider malaria and confirm or rule out this diagnosis.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
